

Characterization of tracheobronchomalacia in infants with hypophosphatasia
- PMID: 32762706
- PMCID: PMC7407429
- DOI: 10.1186/s13023-020-01483-9
Characterization of tracheobronchomalacia in infants with hypophosphatasia
Abstract
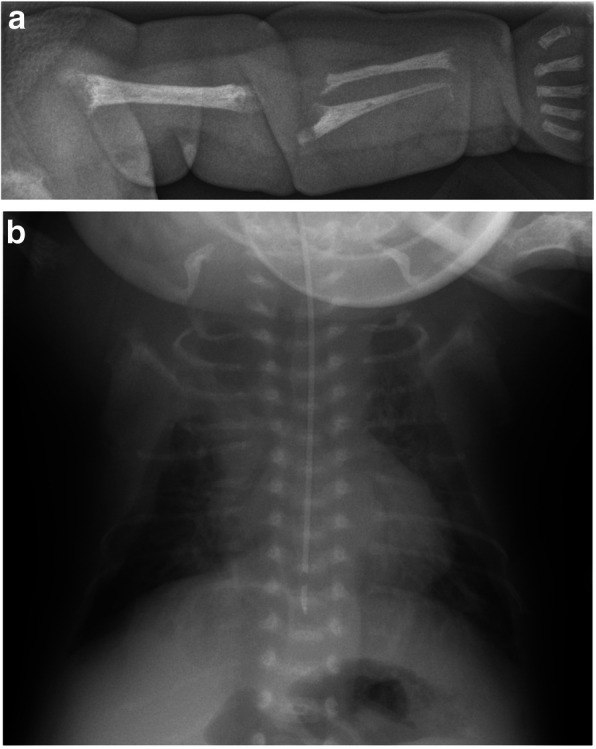
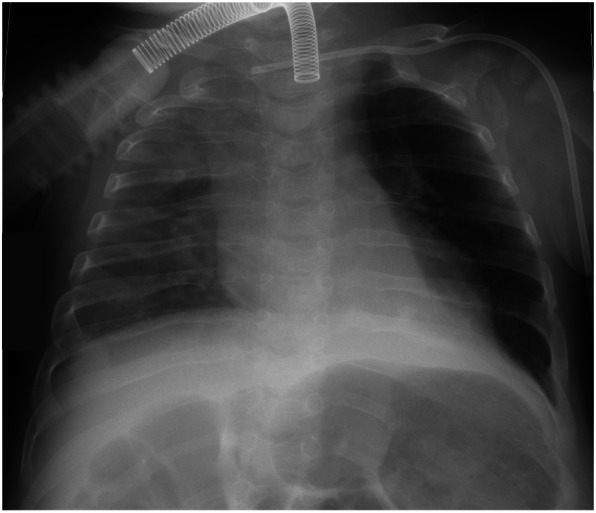
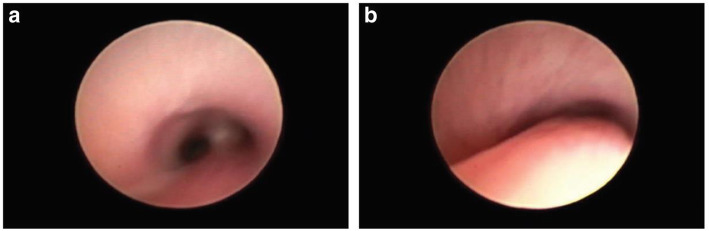
Background: Perinatal and infantile hypophosphatasia (HPP) are associated with respiratory failure and respiratory complications. Effective management of such complications is of key clinical importance. In some infants with HPP, severe tracheobronchomalacia (TBM) contributes to respiratory difficulties. The objective of this study is to characterize the clinical features, investigations and management in these patients.
Methods: We report a case series of five infants with perinatal HPP, with confirmed TBM, who were treated with asfotase alfa and observed for 3-7 years. Additionally, we reviewed respiratory function data in a subgroup of patients with perinatal and infantile HPP included in the clinical trials of asfotase alfa, who required high-pressure respiratory support (positive end-expiratory pressure [PEEP] ≥6 cm H2O and/or peak inspiratory pressure ≥18 cm H2O) during the studies.
Results: The case series showed that TBM contributed significantly to respiratory morbidity, and prolonged respiratory support with high PEEP was required. However, TBM improved over time, allowing weaning of all patients from ventilator use. The review of clinical trial data included 20 patients and found a high degree of heterogeneity in PEEP requirements across the cohort; median PEEP was 8 cm H2O at any time and some patients presented with high PEEP (≥8 cm H2O) over periods of more than 6 months.
Conclusion: In infants with HPP presenting with persistent respiratory complications, it is important to screen for TBM and initiate appropriate respiratory support and treatment with asfotase alfa at an early stage.
Trial registration: ClinicalTrials.gov numbers: NCT00744042 , registered 27 August 2008; NCT01205152 , registered 17 September 2010; NCT01176266 , registered 29 July 2010.
Keywords: Asfotase alfa; Hypophosphatasia; Respiratory failure; Respiratory support; Tracheobronchomalacia.
Conflict of interest statement
RP, HS and RY are members of the Advisory Board for Alexion Pharmaceuticals, Inc. RP and HS are members of the Speakers Bureau for Alexion Pharmaceuticals, Inc. RP, HS and MZM participated as investigators in the clinical trial program for asfotase alfa, which was sponsored by Alexion Pharmaceuticals, Inc. RP, HS, RY and MZM have received honoraria from Alexion Pharmaceuticals, Inc. The other authors have no financial relationships relevant to this article to disclose.
Figures
References
-
- Whyte MP. Hypophosphatasia. In: Thakker RV, Whyte MP, Eisman JA, Igarashi T, editors. Genetics of bone biology and skeletal disease. London: Academic; 2013. pp. 337–360.
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
