

Heart and Lung Multimodality Imaging in COVID-19
- PMID: 32762885
- PMCID: PMC7314453
- DOI: 10.1016/j.jcmg.2020.05.017
Heart and Lung Multimodality Imaging in COVID-19
Abstract
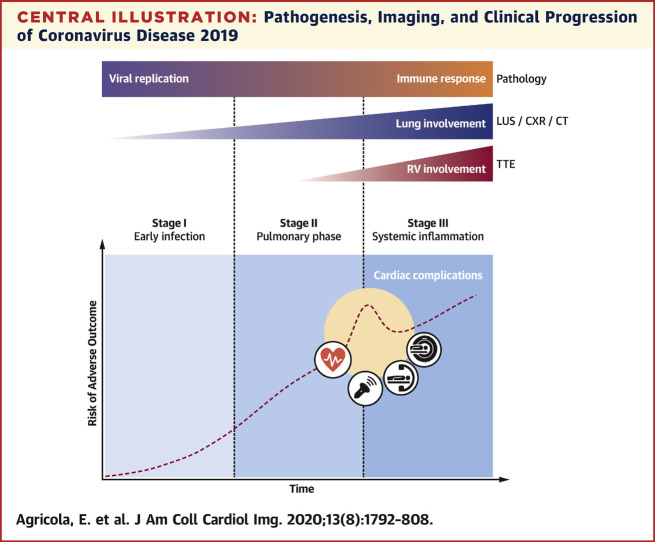
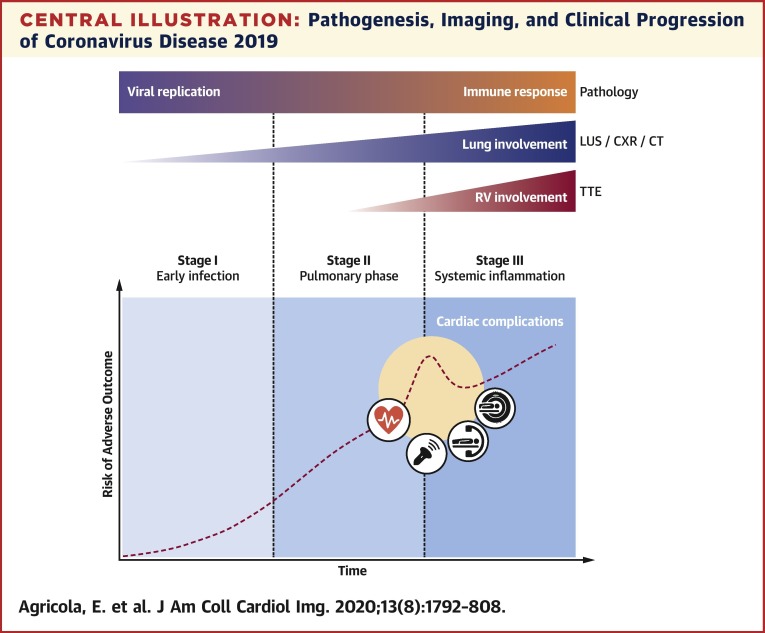
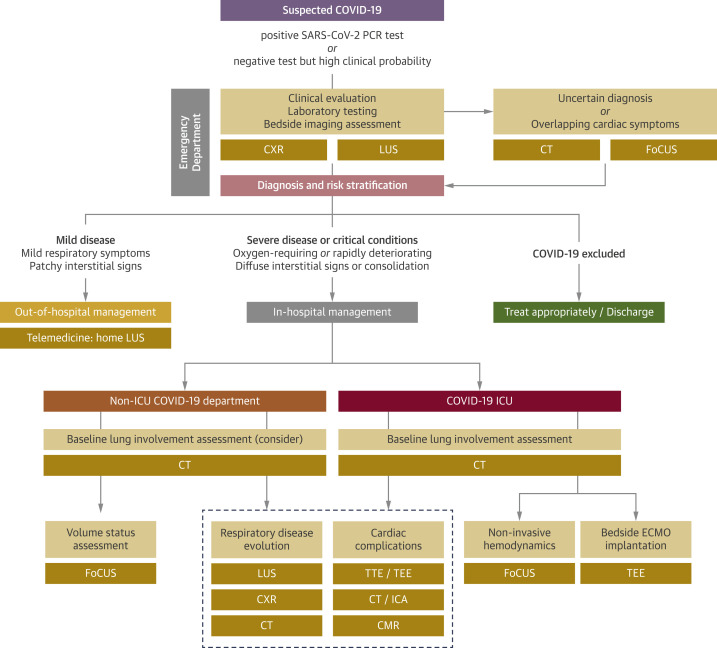
The severe acute respiratory syndrome-coronavirus-2 outbreak has rapidly reached pandemic proportions and has become a major threat to global health. Although the predominant clinical feature of coronavirus disease-2019 (COVID-19) is an acute respiratory syndrome of varying severity, ranging from mild symptomatic interstitial pneumonia to acute respiratory distress syndrome, the cardiovascular system can be involved in several ways. As many as 40% of patients hospitalized with COVID-19 have histories of cardiovascular disease, and current estimates report a proportion of myocardial injury in patients with COVID-19 of up to 12%. Multiple pathways have been suggested to explain this finding and the related clinical scenarios, encompassing local and systemic inflammatory responses and oxygen supply-demand imbalance. From a clinical point of view, cardiac involvement during COVID-19 may present a wide spectrum of severity, ranging from subclinical myocardial injury to well-defined clinical entities (myocarditis, myocardial infarction, pulmonary embolism, and heart failure), whose incidence and prognostic implications are currently largely unknown because of a significant lack of imaging data. Integrated heart and lung multimodality imaging plays a central role in different clinical settings and is essential in the diagnosis, risk stratification, and management of patients with COVID-19. The aims of this review are to summarize imaging-oriented pathophysiological mechanisms of lung and cardiac involvement in COVID-19 and to provide a guide for integrated imaging assessment in these patients.
Keywords: COVID-19; SARS-CoV-2; cardiac magnetic resonance; chest x-ray; computed tomography; coronavirus; echocardiography; lung ultrasound; multimodality imaging.
Copyright © 2020 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Bonow R.O., Fonarow G.C., O’Gara P.T., Yancy C.W. Association of coronavirus disease 2019 (COVID-19) with myocardial injury and mortality. JAMA Cardiol. 2020 Mar 27 [E-pub ahead of print] - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
