

Management of irreparable massive rotator cuff tears: a systematic review and meta-analysis of patient-reported outcomes, reoperation rates, and treatment response
- PMID: 32763381
- PMCID: PMC7669555
- DOI: 10.1016/j.jse.2020.07.030
Management of irreparable massive rotator cuff tears: a systematic review and meta-analysis of patient-reported outcomes, reoperation rates, and treatment response
Abstract
Background: There is no consensus on the treatment of irreparable massive rotator cuff tears. The goal of this systematic review and meta-analysis was to (1) compare patient-reported outcome scores, (2) define failure and reoperation rates, and (3) quantify the magnitude of patient response across treatment strategies.
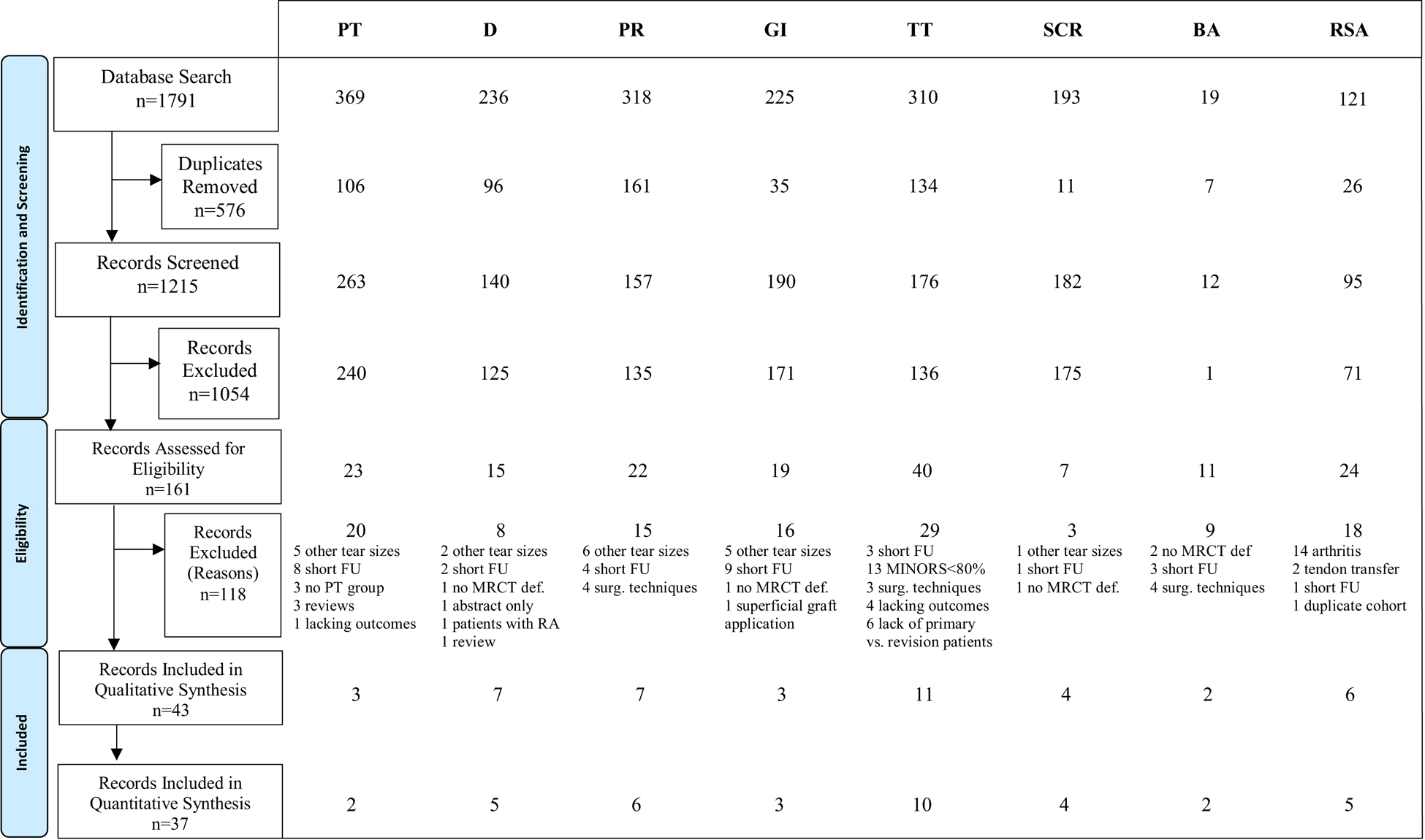
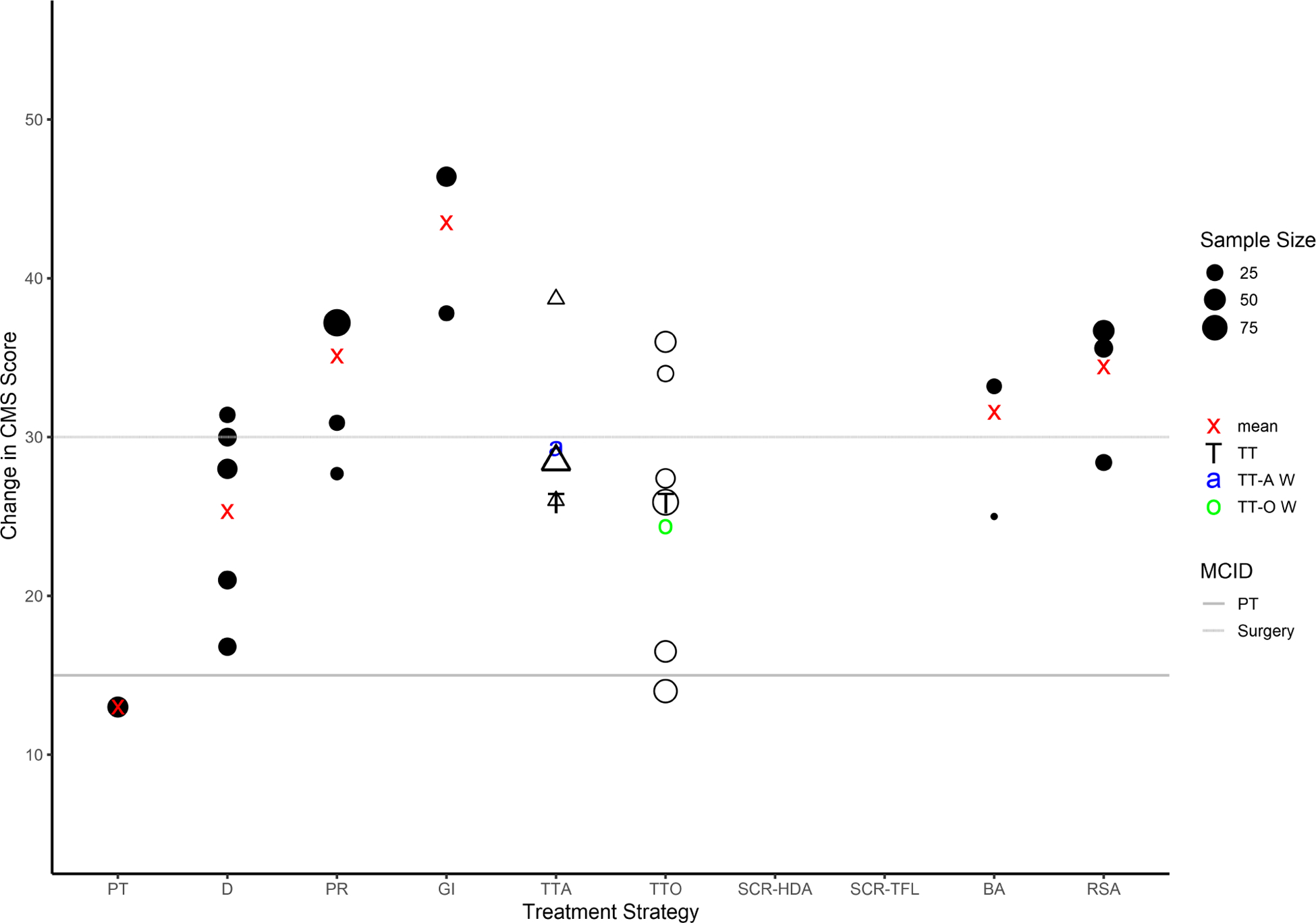
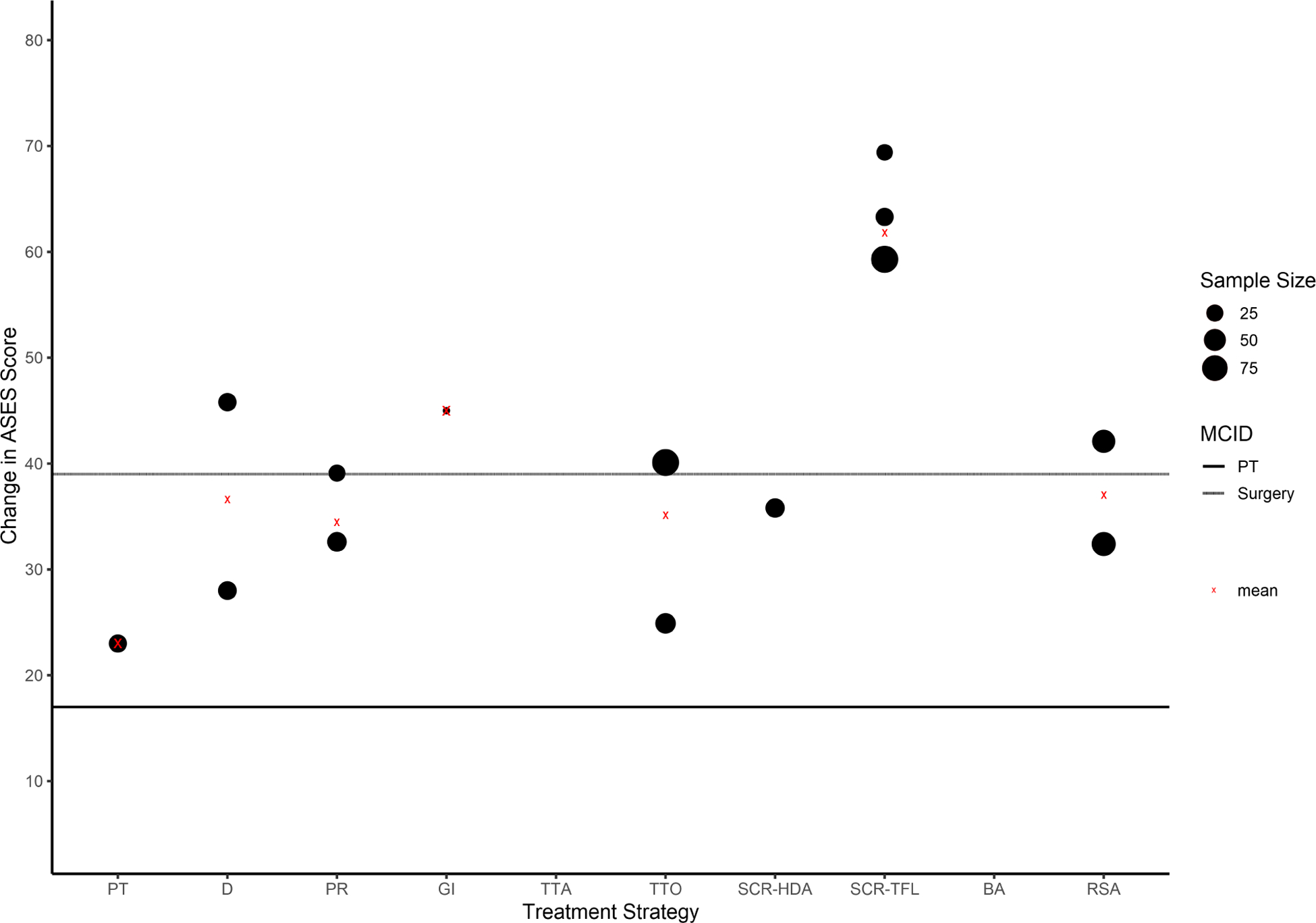
Methods: The MEDLINE, Embase, CENTRAL (Cochrane Central Register of Controlled Trials), and Scopus databases were searched for studies including physical therapy and operative treatment of massive rotator cuff tears. The criteria of the Methodological Index for Non-randomized Studies were used to assess study quality. Primary outcome measures were patient-reported outcome scores as well as failure, complication, and reoperation rates. To quantify patient response to treatment, we compared changes in the Constant-Murley score and American Shoulder and Elbow Surgeons (ASES) score with previously reported minimal clinically important difference (MCID) thresholds.
Results: No level I or II studies that met the inclusion and exclusion criteria were found. Physical therapy was associated with a 30% failure rate among the included patients, and another 30% went on to undergo surgery. Partial repair was associated with a 45% retear rate and 10% reoperation rate. Only graft interposition was associated with a weighted average change that exceeded the MCID for both the Constant-Murley score and ASES score. Latissimus tendon transfer techniques using humeral bone tunnel fixation were associated with a 77% failure rate. Superior capsular reconstruction with fascia lata autograft was associated with a weighted average change that exceeded the MCID for the ASES score. Reverse arthroplasty was associated with a 10% prosthesis failure rate and 8% reoperation rate.
Conclusion: There is a lack of high-quality comparative studies to guide treatment recommendations. Compared with surgery, physical therapy is associated with less improvement in perceived functional outcomes and a higher clinical failure rate.
Keywords: Irreparable massive rotator cuff tear; complications; failure rate; meta-analysis; patient-reported outcomes; reoperation; response to treatment; systematic review.
Copyright © 2020 Journal of Shoulder and Elbow Surgery Board of Trustees. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflicts of interest/Disclosures:
Figures
References
-
- American Academy of Orthopaedic Surgeons. Management of rotator cuff injuries clinical practice guideline. In. https://www.aaos.org/globalassets/quality-and-practice-resources/rotator... - PubMed
-
- Burkhart SS, Danaceau SM, Pearce CE Jr. Arthroscopic rotator cuff repair: analysis of results by tear size and by repair technique—margin convergence versus direct tendon-to-bone repair. Arthroscopy 2001;17:905–912. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
