

Sex, age, and hospitalization drive antibody responses in a COVID-19 convalescent plasma donor population
- PMID: 32764200
- PMCID: PMC7598041
- DOI: 10.1172/JCI142004
Sex, age, and hospitalization drive antibody responses in a COVID-19 convalescent plasma donor population
Abstract
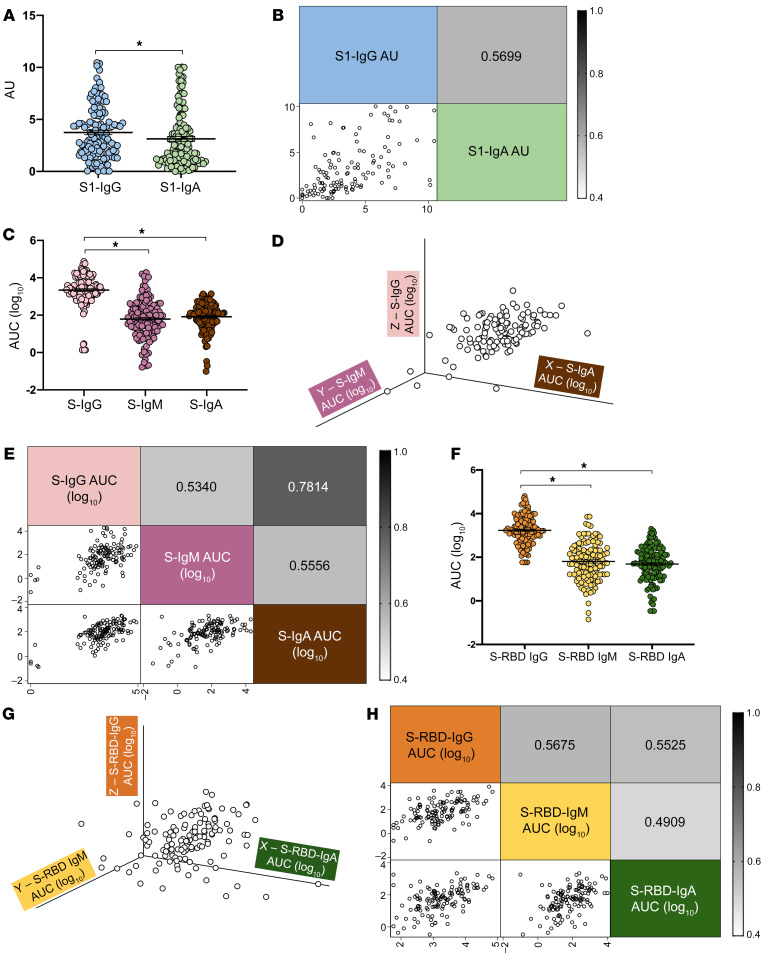
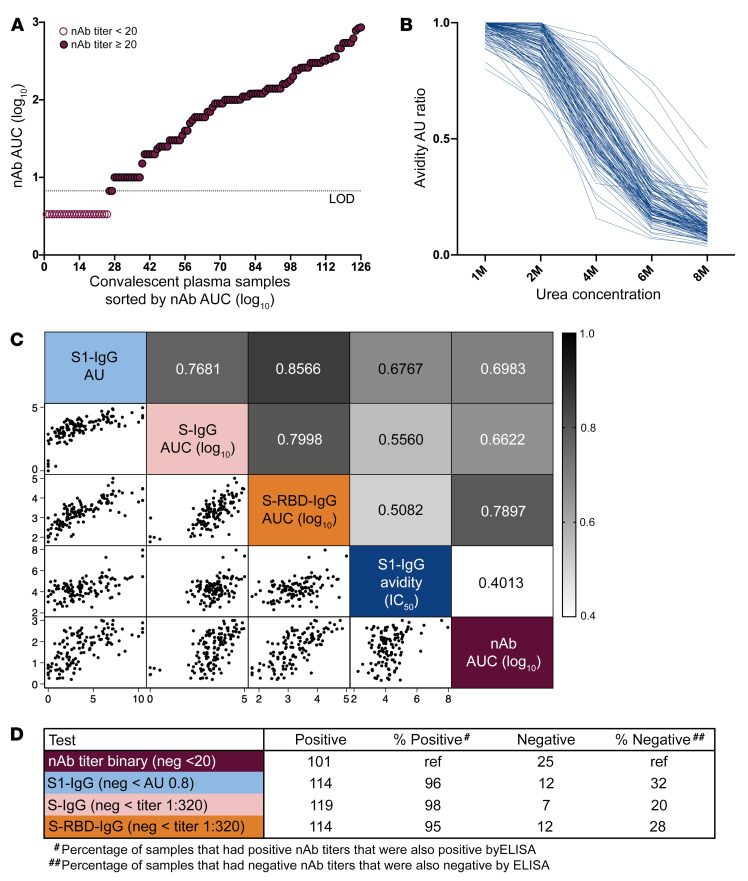
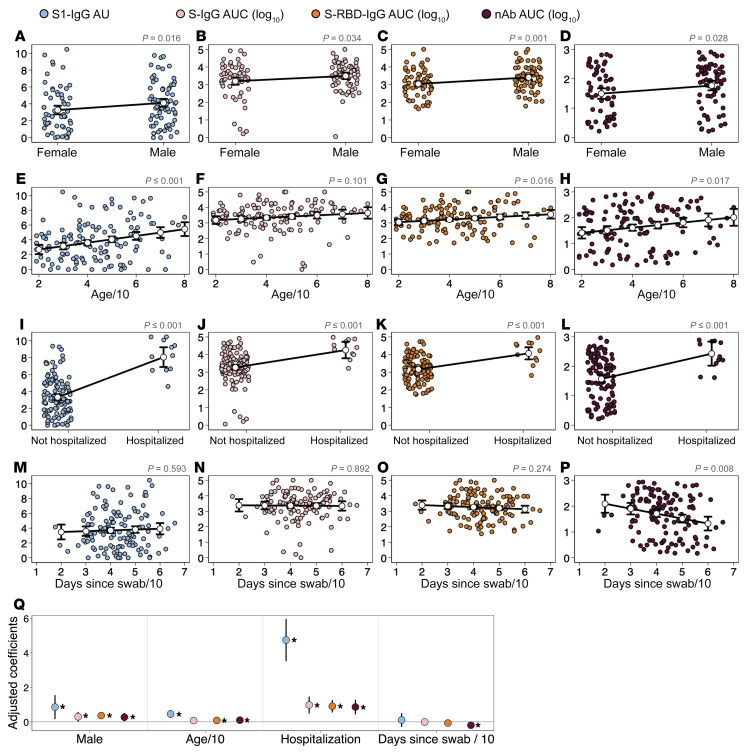
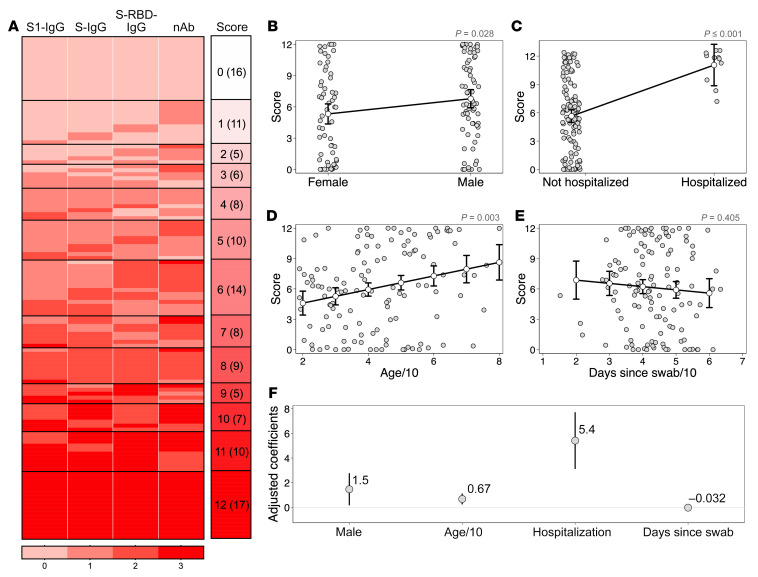
Convalescent plasma is a leading treatment for coronavirus disease 2019 (COVID-19), but there is a paucity of data identifying its therapeutic efficacy. Among 126 potential convalescent plasma donors, the humoral immune response was evaluated using a severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) virus neutralization assay with Vero-E6-TMPRSS2 cells; a commercial IgG and IgA ELISA to detect the spike (S) protein S1 domain (EUROIMMUN); IgA, IgG, and IgM indirect ELISAs to detect the full-length S protein or S receptor-binding domain (S-RBD); and an IgG avidity assay. We used multiple linear regression and predictive models to assess the correlations between antibody responses and demographic and clinical characteristics. IgG titers were greater than either IgM or IgA titers for S1, full-length S, and S-RBD in the overall population. Of the 126 plasma samples, 101 (80%) had detectable neutralizing antibody (nAb) titers. Using nAb titers as the reference, the IgG ELISAs confirmed 95%-98% of the nAb-positive samples, but 20%-32% of the nAb-negative samples were still IgG ELISA positive. Male sex, older age, and hospitalization for COVID-19 were associated with increased antibody responses across the serological assays. There was substantial heterogeneity in the antibody response among potential convalescent plasma donors, but sex, age, and hospitalization emerged as factors that can be used to identify individuals with a high likelihood of having strong antiviral antibody responses.
Keywords: COVID-19; Immunoglobulins.
Conflict of interest statement
Figures
Update of
-
Sex, age, and hospitalization drive antibody responses in a COVID-19 convalescent plasma donor population.medRxiv [Preprint]. 2020 Jun 28:2020.06.26.20139063. doi: 10.1101/2020.06.26.20139063. medRxiv. 2020. Update in: J Clin Invest. 2020 Nov 2;130(11):6141-6150. doi: 10.1172/JCI142004. PMID: 32607519 Free PMC article. Updated. Preprint.
References
-
- JHU. Johns Hopkins University Coronavirus Resource Center. https://coronavirus.jhu.edu/map.html Accessed 10/6/2020.
Publication types
MeSH terms
Substances
Grants and funding
- R01 AI152078/AI/NIAID NIH HHS/United States
- T32 GM136577/GM/NIGMS NIH HHS/United States
- R01 AI120938/AI/NIAID NIH HHS/United States
- T32 CA009110/CA/NCI NIH HHS/United States
- U54 AG062333/AG/NIA NIH HHS/United States
- R01 AI052733/AI/NIAID NIH HHS/United States
- R01 AI128779/AI/NIAID NIH HHS/United States
- R01 NR005228/NR/NINR NIH HHS/United States
- HHSN272201400007C/AI/NIAID NIH HHS/United States
- K23 HL151826/HL/NHLBI NIH HHS/United States
- T32 AI007417/AI/NIAID NIH HHS/United States
- R01 HL059842/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
