

Post-stroke Cognitive Impairment-Impact of Follow-Up Time and Stroke Subtype on Severity and Cognitive Profile: The Nor-COAST Study
- PMID: 32765406
- PMCID: PMC7379332
- DOI: 10.3389/fneur.2020.00699
Post-stroke Cognitive Impairment-Impact of Follow-Up Time and Stroke Subtype on Severity and Cognitive Profile: The Nor-COAST Study
Abstract
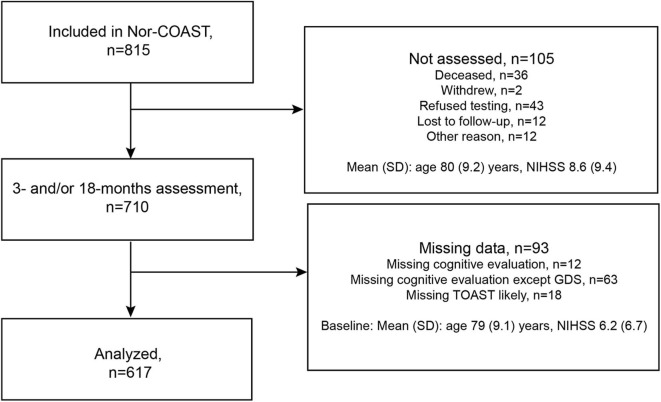
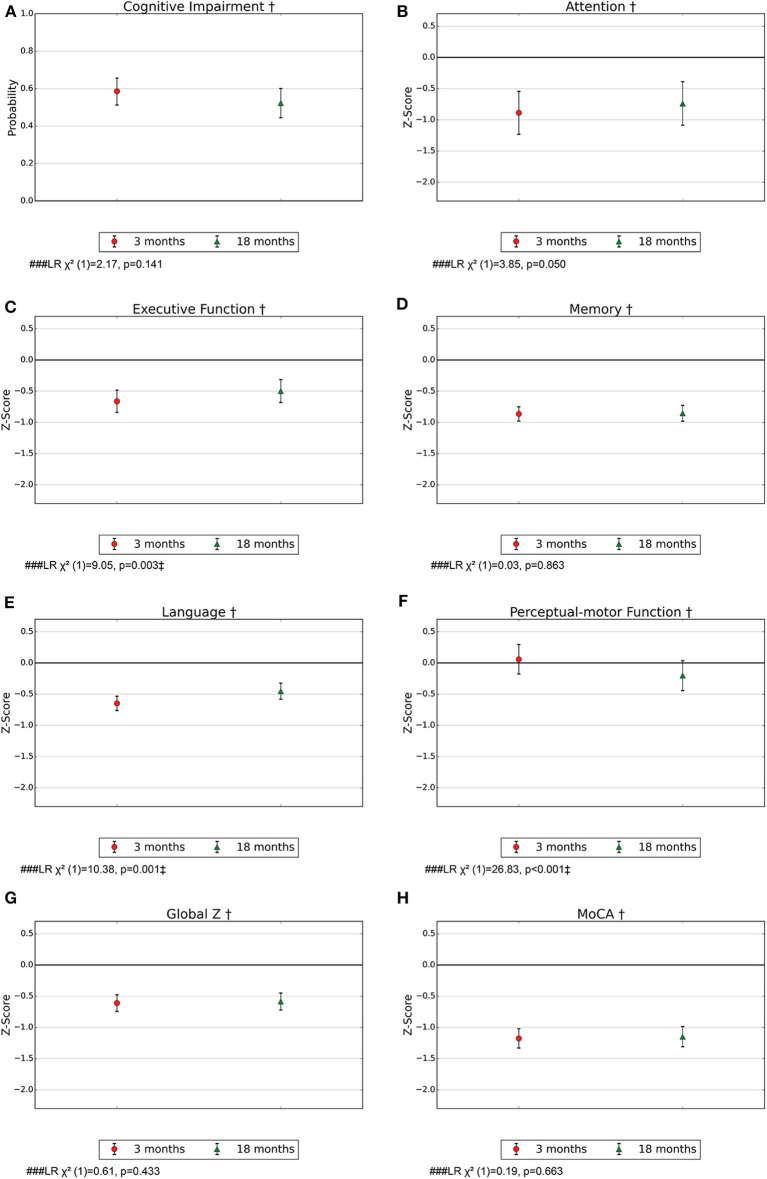
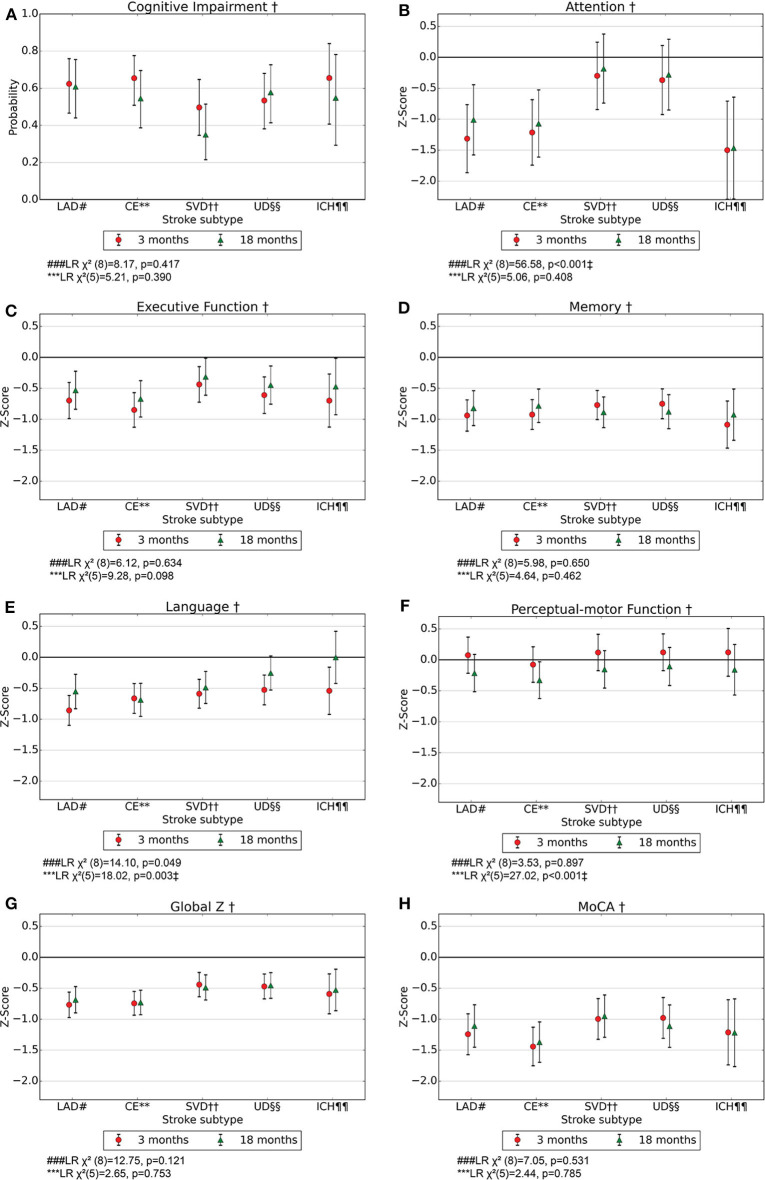
Background: Post-stroke cognitive impairment (PSCI) is common, but evidence of cognitive symptom profiles, course over time, and pathogenesis is scarce. We investigated the significance of time and etiologic stroke subtype for the probability of PSCI, severity, and cognitive profile. Methods: Stroke survivors (n = 617) underwent cognitive assessments of attention, executive function, memory, language, perceptual-motor function, and the Montreal Cognitive Assessment (MoCA) after 3 and/or 18 months. PSCI was classified according to DSM-5 criteria. Stroke severity was assessed with the National Institutes of Health Stroke Scale (NIHSS). Stroke subtype was categorized as intracerebral hemorrhage (ICH), large artery disease (LAD), cardioembolic stroke (CE), small vessel disease (SVD), or un-/other determined strokes (UD). Mixed-effects logistic or linear regression was applied with PSCI, MoCA, and z-scores of the cognitive domains as dependent variables. Independent variables were time as well as stroke subtype, time, and interaction between these. The analyses were adjusted for age, education, and sex. The effects of time and stroke subtype were analyzed by likelihood ratio tests (LR). Results: Mean age was 72 years (SD 12), 42% were females, and mean NIHSS score at admittance was 3.8 (SD 4.8). Probability (95% CI) for PSCI after 3 and 18 months was 0.59 (0.51-0.66) and 0.51 (0.52-0.60), respectively and remained constant over time. Global measures and most cognitive domains were assessed as impaired for the entire stroke population and for most stroke subtypes. Executive function and language improved for the entire stroke population (LR) = 9.05, p = 0.003, and LR = 10.38, p = 0.001, respectively). After dividing the sample according to stroke subtypes, language improved for ICH patients (LR = 18.02, p = 0.003). No significant differences were found in the severity of impairment between stroke subtypes except for attention, which was impaired for LAD and CE in contrast to no impairment for SVD (LR = 56.58, p < 0.001). Conclusions: In this study including mainly minor strokes, PSCI is common for all subtypes, both early and long-term after stroke, while executive function and language improve over time. The findings might contribute to personalizing follow-up and offer new insights into underlying mechanisms. Further research is needed on underlying mechanisms, PSCI prevention and treatment, and relevance for rehabilitation.
Keywords: cerebrovascular disease; cognitive domains; intracerebral hemorrhag; post-stroke cognitive impairment; prognosis; stroke; stroke subtype; vascular dementia.
Copyright © 2020 Aam, Einstad, Munthe-Kaas, Lydersen, Ihle-Hansen, Knapskog, Ellekjær, Seljeseth and Saltvedt.
Figures
References
-
- Hay SI, Abajobir AA, Abate KH, Abbafati C, Abbas KM, Abd-Allah F, et al. Global, regional, and national disability-adjusted life-years (DALYs) for 333 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. (2017) 390:1260–344. 10.1016/S0140-6736(17)32130-X - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources