

Paracetamol vs. Ibuprofen in Preterm Infants With Hemodynamically Significant Patent Ductus Arteriosus: A Non-inferiority Randomized Clinical Trial Protocol
- PMID: 32766181
- PMCID: PMC7380081
- DOI: 10.3389/fped.2020.00372
Paracetamol vs. Ibuprofen in Preterm Infants With Hemodynamically Significant Patent Ductus Arteriosus: A Non-inferiority Randomized Clinical Trial Protocol
Erratum in
-
Corrigendum: Paracetamol vs. Ibuprofen in Preterm Infants With Hemodynamically Significant Patent Ductus Arteriosus: A Non-inferiority Randomized Clinical Trial Protocol.Front Pediatr. 2022 Jan 13;9:834454. doi: 10.3389/fped.2021.834454. eCollection 2021. Front Pediatr. 2022. PMID: 35096721 Free PMC article.
Abstract
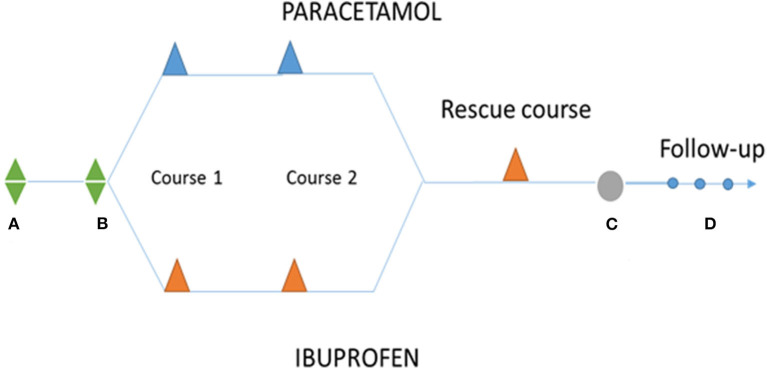
Background: Currently, the first line treatment of persistent ductus arteriosus (PDA) is either indomethacin or ibuprofen. However, the potentially life-threatening side effects associated to their use have prompted physicians to look for alternative options. The incorporation of paracetamol as an alternative to ibuprofen in the management of PDA is still based on insufficient clinical evidence. Hence, more clinical trials are needed to establish a therapeutic role for paracetamol in the management of PDA that take into consideration short- and long-term safety and efficacy outcomes. Study Design: This is a non-inferiority, randomized, multicenter, double-blinded study to evaluate the efficacy, and safety of intravenous (IV) paracetamol vs. IV ibuprofen (standard treatment) for PDA in preterm patients with a gestational age ≤ 30 weeks. At baseline, patients will be randomized (1:1) to treatment with paracetamol or ibuprofen. The primary endpoint is closure of the ductus after the first treatment course. Secondary endpoints are related to effectiveness (need for a second treatment course, rescue treatment, reopening rate, time to definitive closure, need for surgical ligation), safety (early and long-term complications), pharmacokinetics, and pharmacodynamics, pharmacogenetics, pharmacoeconomics, and genotoxicity. Long-term follow-up to 24 months of corrected postnatal age will be performed using Bayley III neurodevelopmental scale. Trial Registration: ClinicalTrials.gov Identifier: NCT04037514. EudraCT: 2015-003177-14.
Keywords: ductus; efficacy; paracetamol; pharmacogenetics; pharmacokinetics; safety.
Copyright © 2020 García-Robles, Gimeno Navarro, Serrano Martín, Párraga Quiles, Parra Llorca, Poveda-Andrés, Vento Torres and Aguar Carrascosa.
Figures
References
-
- González MDR, Guzmán EG, Quiles MJP, Tejero MA, Cabañas JMG. Ductus arterioso persistente. Protoc Diagnóstico Ter AEP Neonatol. (2008) 353–361.