

Trends in Disease Burden Attributable to Tobacco in China, 1990-2017: Findings From the Global Burden of Disease Study 2017
- PMID: 32766191
- PMCID: PMC7381278
- DOI: 10.3389/fpubh.2020.00237
Trends in Disease Burden Attributable to Tobacco in China, 1990-2017: Findings From the Global Burden of Disease Study 2017
Abstract
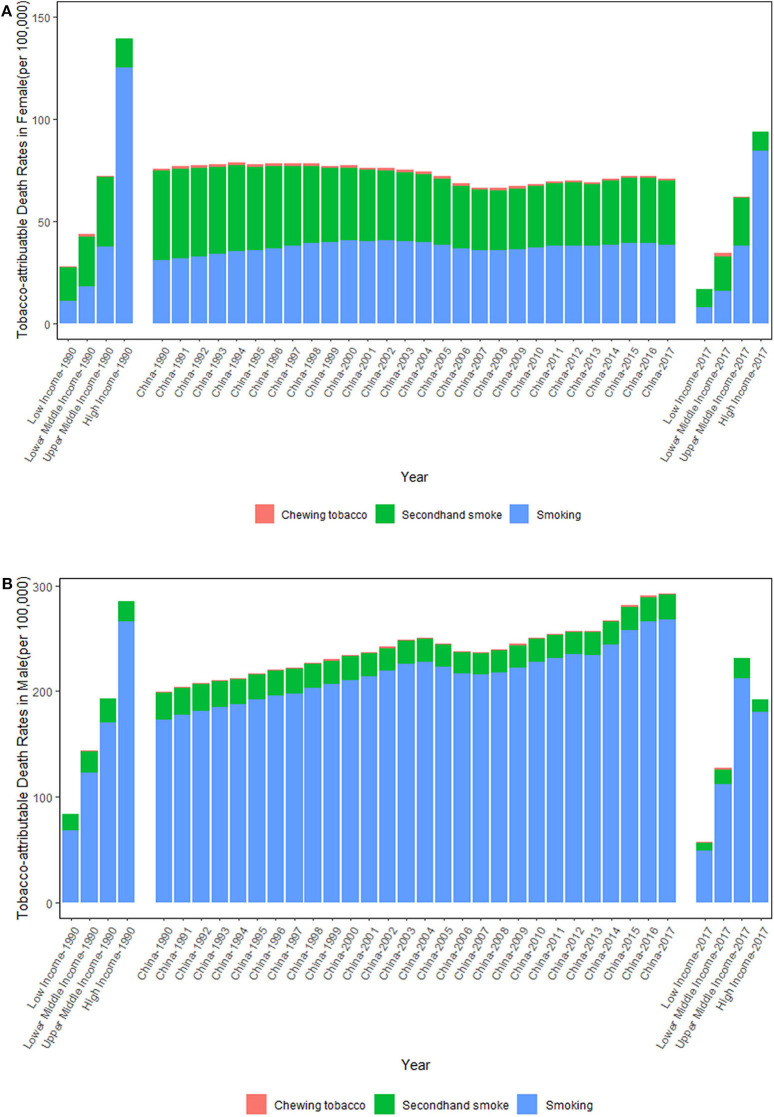
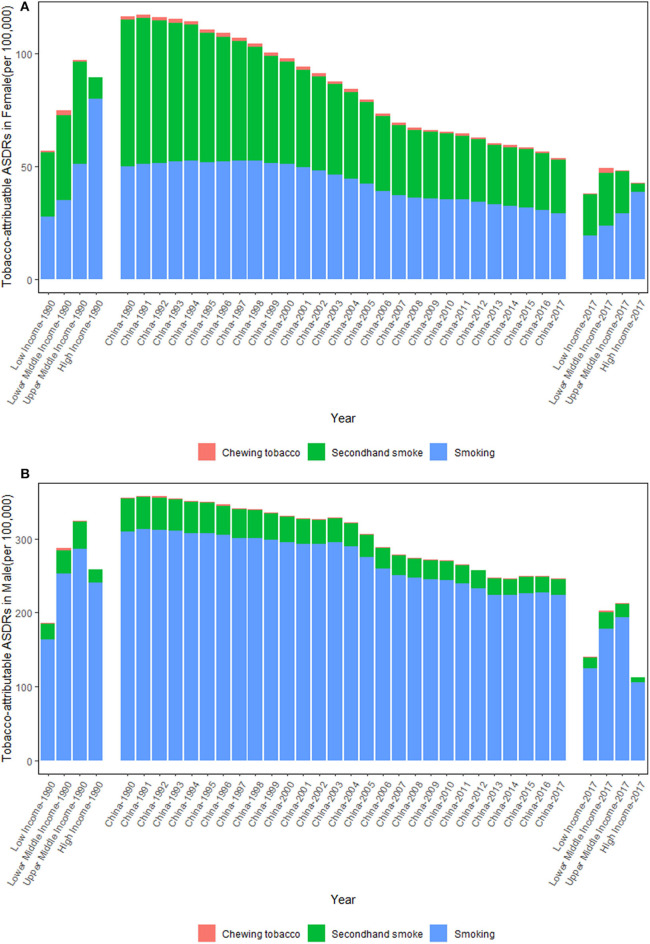
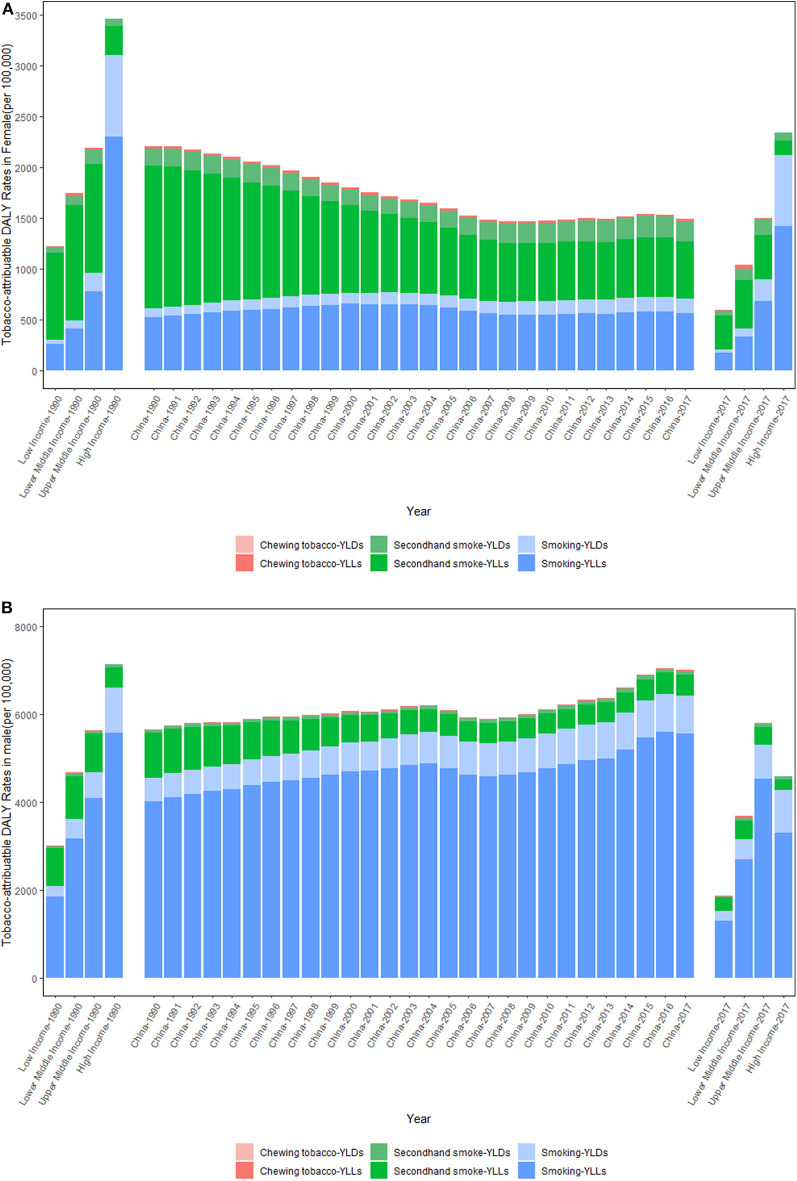
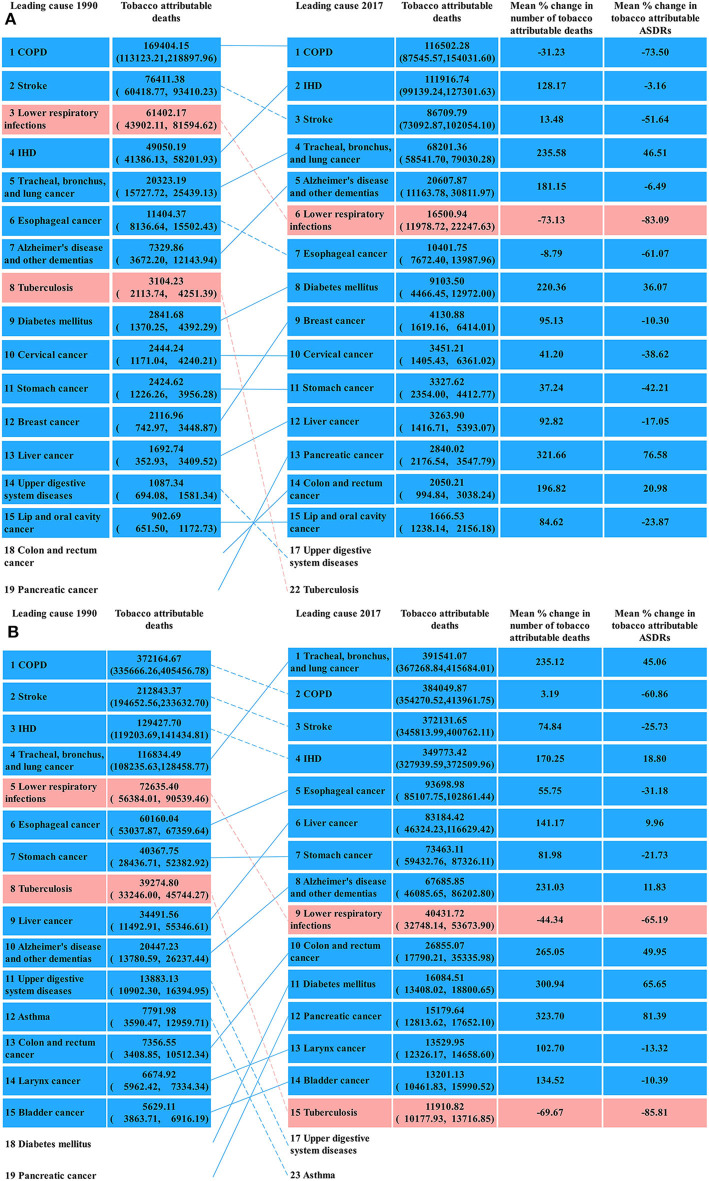
In 2018, there were more than 371 million cigarette smokers and 12. 6 million electronic cigarette users, with 340.2 million non-smokers exposed to secondhand smoke (SHS) in China, which resulted in heavy tobacco-attributable disease burden. According to the definition by the Global Burden of Disease Study 2017 (GBD 2017), tobacco is a level 2 risk factor that consists of three sublevel risk factors, namely, smoking, SHS, and chewing tobacco. In this study, we aimed to evaluate the trends in deaths and disability-adjusted life years (DALYs) attributable to tobacco, smoking, SHS, and chewing tobacco by sex in China from 1990 to 2017 and to explore the leading causes of tobacco-attributable deaths and DALYs using data from the GBD 2017. From 1990 to 2017, the tobacco-attributable death rates per 100,000 people decreased from 75.65 [95% uncertainty interval (95% UI) = 56.23-97.74] to 70.90 (95% UI = 59.67-83.72) in females and increased from 198.83 (95% UI = 181.39-217.47) to 292.39 (95% UI = 271.28-313.76) in males. From 1990 to 2017, the tobacco-attributable DALY rates decreased from 2209.11 (95% UI = 1678.63-2791.91) to 1489.05 (95% UI = 1237.65-1752.57) in females and increased from 5650.42 (95% UI = 5070.06-6264.39) to 6994.02 (95% UI = 6489.84-7558.41) in males. In 2017, the tobacco-attributable deaths in China were concentrated on chronic obstructive pulmonary disease, ischemic heart disease, lung cancer, and stroke. The focus of tobacco control for females was SHS in 1990, whereas smoking and SHS were equally important for tobacco control in females in 2017. Increasing tobacco taxes and prices may be the most effective and feasible measure to reduce tobacco-attributable disease burdens.
Keywords: chewing tobacco; deaths; disability-adjusted life years; global burden of disease; secondhand smoke; smoking; tobacco.
Copyright © 2020 Wen, Xie, Wang, Wu and Yu.
Figures

References
-
- GBD 2017 Risk Factor Collaborators. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. (2018) 392:1923. 10.1016/S0140-6736(18)32225-6 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources