

Lung Involvement in Primary Sjögren's Syndrome-An Under-Diagnosed Entity
- PMID: 32766261
- PMCID: PMC7378373
- DOI: 10.3389/fmed.2020.00332
Lung Involvement in Primary Sjögren's Syndrome-An Under-Diagnosed Entity
Abstract
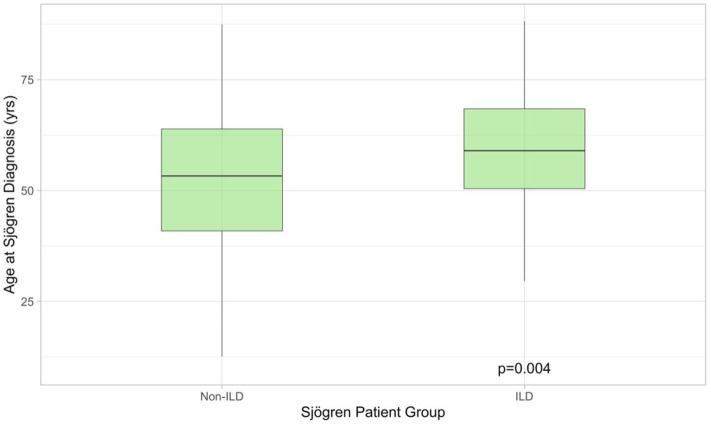
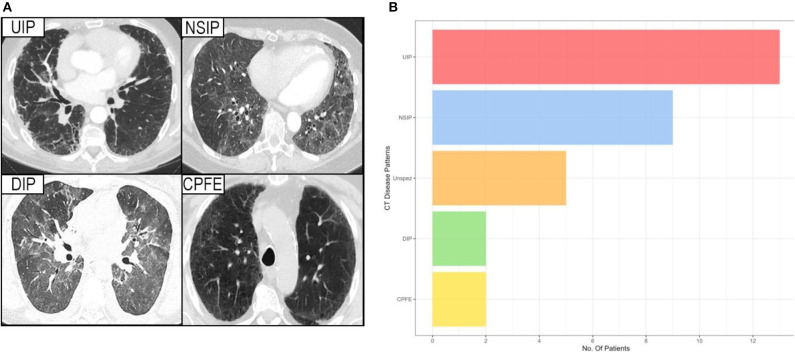
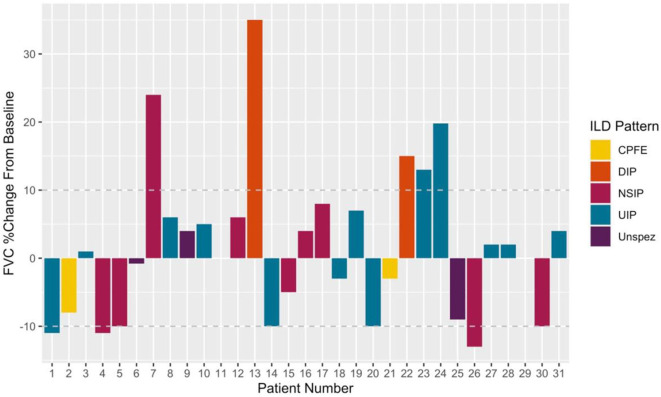
Interstitial lung disease (ILD) represents a frequent extra-glandular manifestation of primary Sjögren's Syndrome (pSS). Limited published data regarding phenotyping and treatment exists. Advances in managing specific ILD phenotypes have not been comprehensively explored in patients with coexisting pSS. This retrospective study aimed to phenotype lung diseases occurring in a well-described pSS-ILD cohort and describe treatment course and outcomes. Between April 2018 and February 2020, all pSS patients attending our Outpatient clinic were screened for possible lung involvement. Clinical, laboratory and high-resolution computed tomography (HRCT) findings were analyzed. Patients were classified according to HRCT findings into five groups: usual interstitial pneumonia (UIP), non-specific interstitial pneumonia (NSIP), desquamative interstitial pneumonia (DIP), combined pulmonary fibrosis and emphysema (CPFE), and non-specific-ILD. Lung involvement was confirmed in 31/268 pSS patients (13%). One-third (10/31) of pSS-ILD patients were Ro/SSA antibody negative. ILD at pSS diagnosis was present in 19/31 (61%) patients. The commonest phenotype was UIP n = 13 (43%), followed by NSIP n = 9 (29%), DIP n = 2 (6 %), CPFE n = 2 (6 %), and non-specific-ILD n = 5 (16%). Forced vital capacity (FVC) and carbon monoxide diffusion capacity (DLCO) appeared lower in UIP and DIP, without reaching a significant difference. Treatment focused universally on intensified immunosuppression, with 13/31 patients (42%) receiving cyclophosphamide. No anti-fibrotic treatments were used. Median follow-up was 38.2 [12.4-119.6] months. Lung involvement in pSS is heterogeneous. Better phenotyping and tailored treatment may improve outcomes and requires further evaluation in larger prospective studies.
Keywords: ESSDAI—EULAR Sjögren's Syndrome Disease Activity Index; Sjögren's Syndrome (SS); interstitial lung disease (ILD); lung fibrosis; sicca syndrome.
Copyright © 2020 Sogkas, Hirsch, Olsson, Hinrichs, Thiele, Seeliger, Skripuletz, Schmidt, Witte, Jablonka and Ernst.
Figures
References
-
- Fairfax AJ, Haslam PL, Pavia D, Sheahan NF, Bateman JR, Agnew JE, et al. . Pulmonary disorders associated with sjogren's syndrome. Q J Med. (1981) 50:279–95. - PubMed
-
- Dong X, Zhou J, Guo X, Li Y, Xu Y, Fu Q, et al. A retrospective analysis of distinguishing features of chest HRCT and clinical manifestation in primary sjogren's syndrome-related interstitial lung disease in a Chinese population. Clin Rheumatol. (2018) 37:2981–8. 10.1007/s10067-018-4289-6 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous