

Cellular Mechanisms of Rejection of Optic and Sciatic Nerve Transplants: An Observational Study
- PMID: 32766437
- PMCID: PMC7382554
- DOI: 10.1097/TXD.0000000000001012
Cellular Mechanisms of Rejection of Optic and Sciatic Nerve Transplants: An Observational Study
Abstract
Background: Organ transplantation is a standard therapeutic strategy for irreversible organ damage, but the utility of nerve transplantation remains generally unexplored, despite its potential benefit to a large patient population. Here, we aimed to establish a feasible preclinical mouse model for understanding the cellular mechanisms behind the rejection of peripheral and optic nerves.
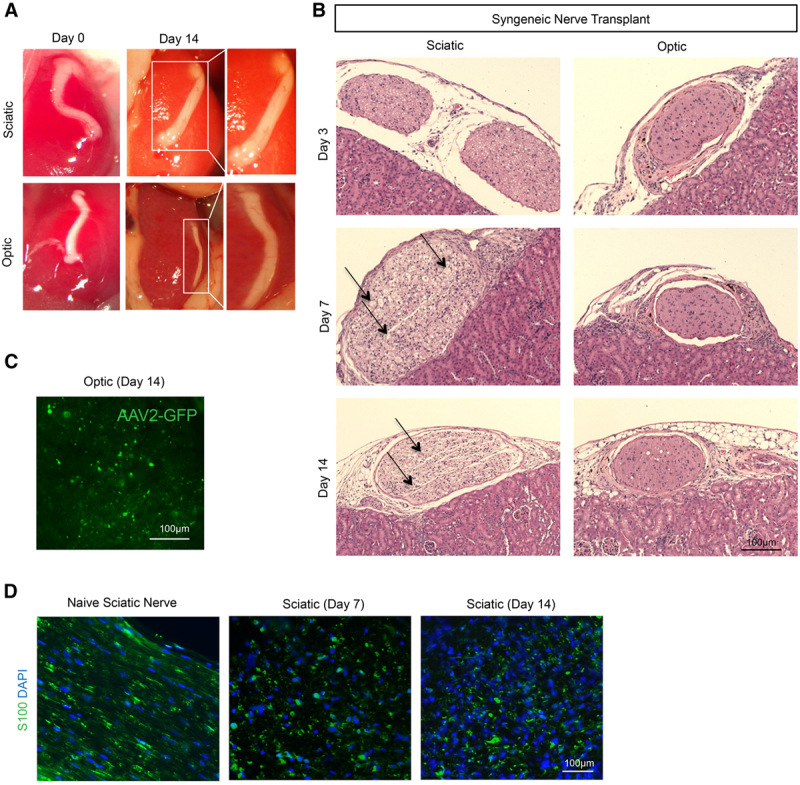
Methods: We performed syngenic and allogenic transplantation of optic and sciatic nerves in mice by inserting the nerve grafts inside the kidney capsule, and we assessed the allografts for signs of rejection through 14 d following transplantation. Then, we assessed the efficacy of CTLA4 Ig, Rapamycin, and anti-CD3 antibody in suppressing immune cell infiltration of the nerve allografts.
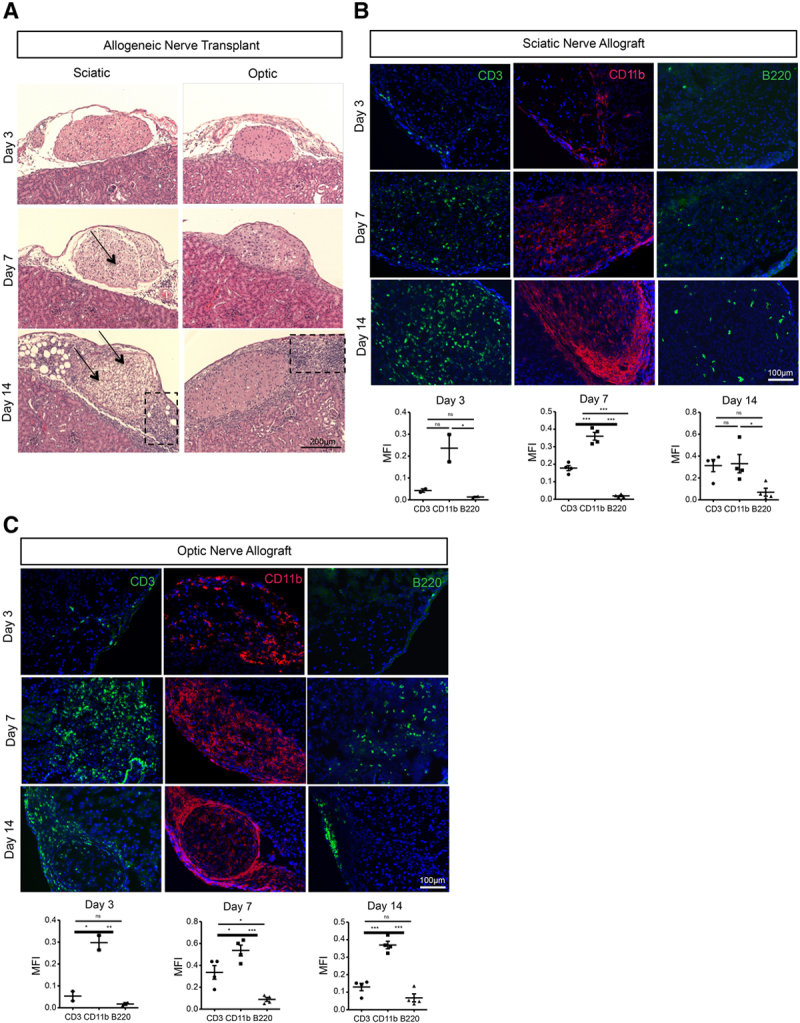
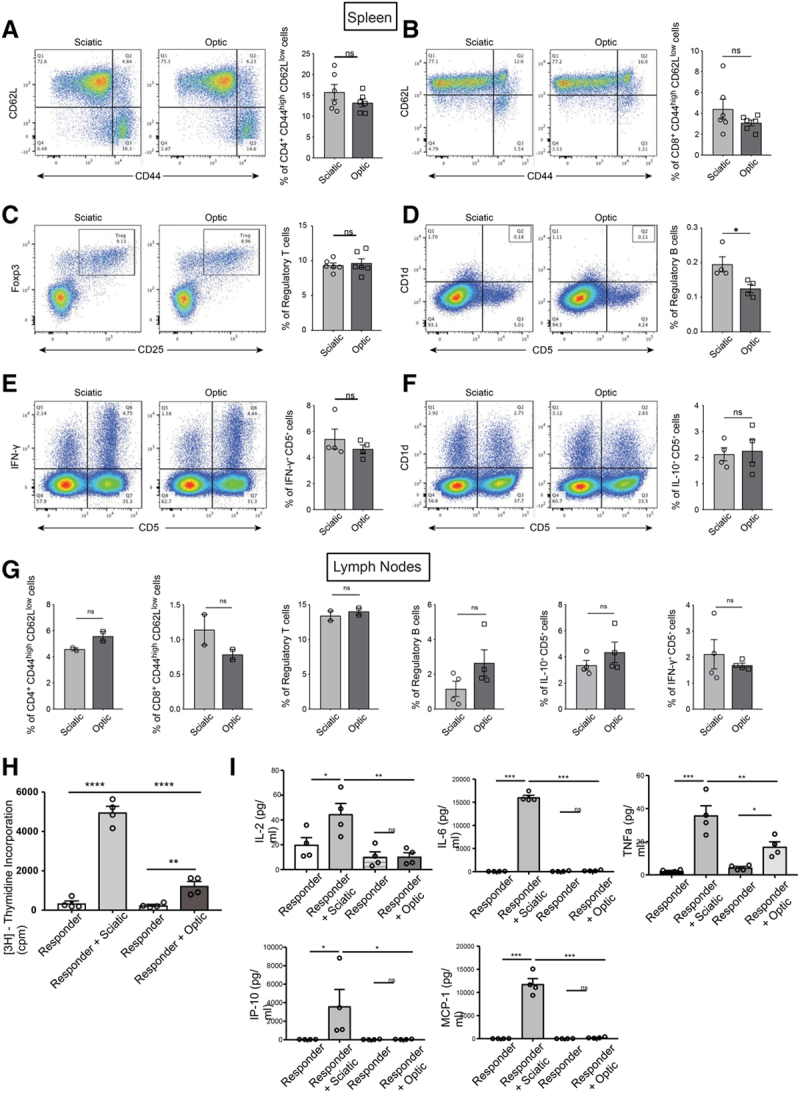
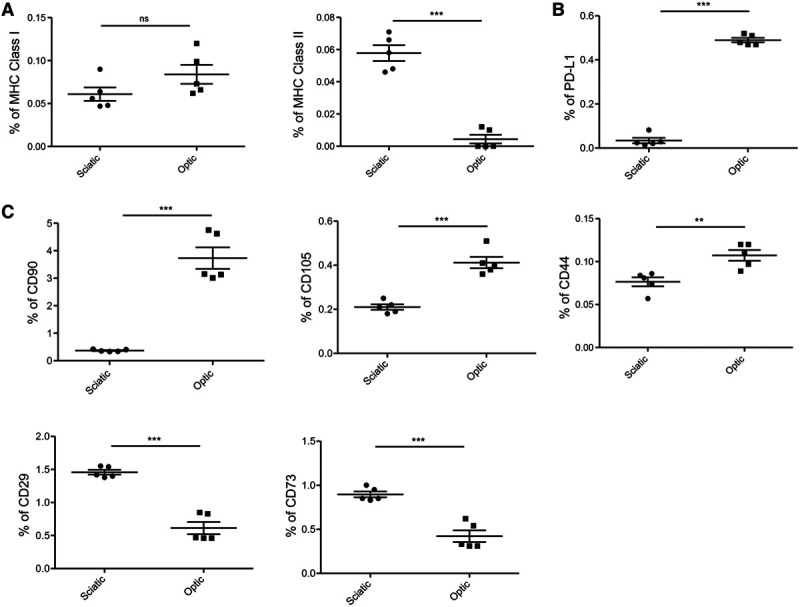
Results: By 3 d posttransplantation, both sciatic and optic nerves transplanted from BALB/c mice into C57BL/6J recipients contained immune cell infiltrates, which included more CD11b+ macrophages than CD3+ T cells or B220+ B cells. Ex vivo immunogenicity assays demonstrated that sciatic nerves demonstrated higher alloreactivity in comparison with optic nerves. Interestingly, optic nerves contained higher populations of anti-inflammatory PD-L1+ cells than sciatic nerves. Treatment with anti-CD3 antibody reduced immune cell infiltrates in the optic nerve allograft, but exerted no significant effect in the sciatic nerve allograft.
Conclusions: These findings establish the feasibility of a preclinical allogenic nerve transplantation model and provide the basis for future testing of directed, high-intensity immunosuppression in these mice.
Copyright © 2020 The Author(s). Transplantation Direct. Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures

References
-
- Taylor DO, Edwards LB, Mohacsi PJ, et al. The registry of the International Society for Heart and Lung Transplantation: twentieth official adult heart transplant report–2003. J Heart Lung Transplant. 2003; 22:616–624. doi:10.1016/s1053-2498(03)00186-4 - PubMed
