

Enabling the assessment of trauma-induced hemorrhage via smart wearable systems
- PMID: 32766449
- PMCID: PMC7375804
- DOI: 10.1126/sciadv.abb1708
Enabling the assessment of trauma-induced hemorrhage via smart wearable systems
Abstract
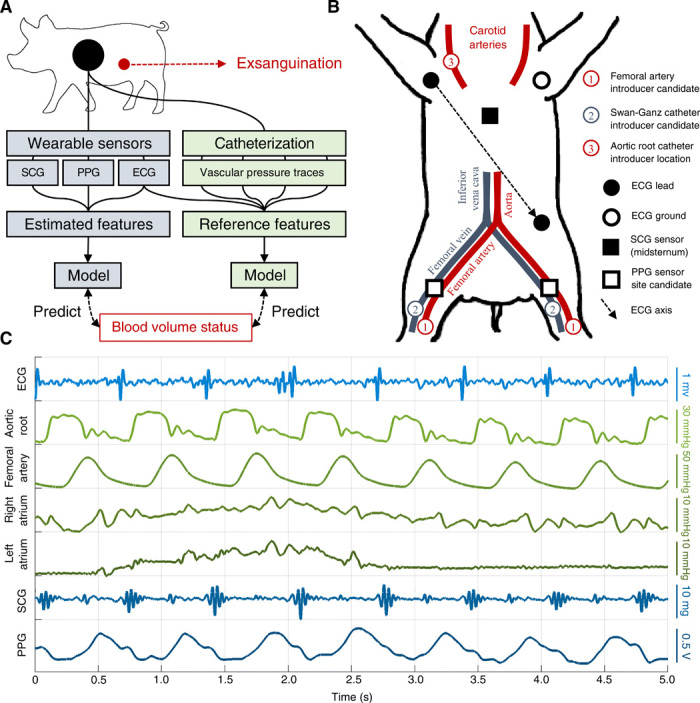
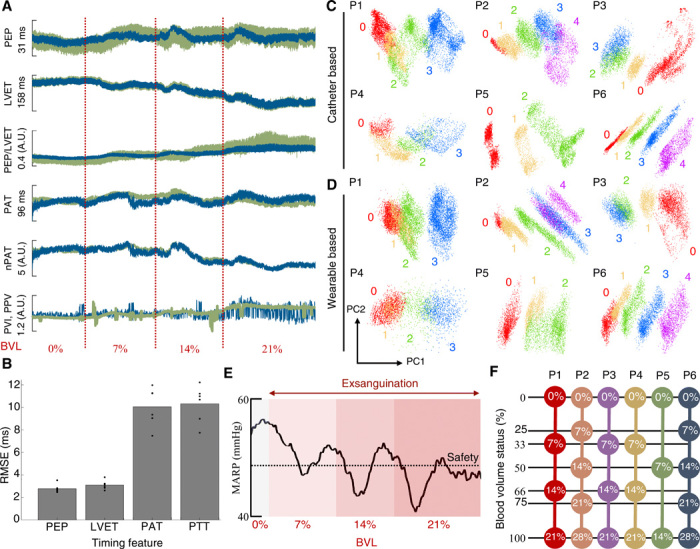
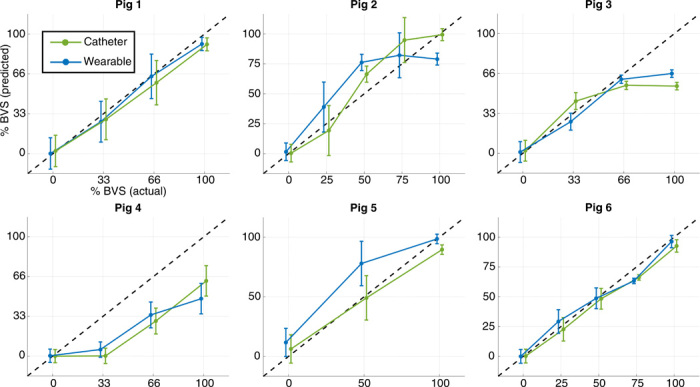
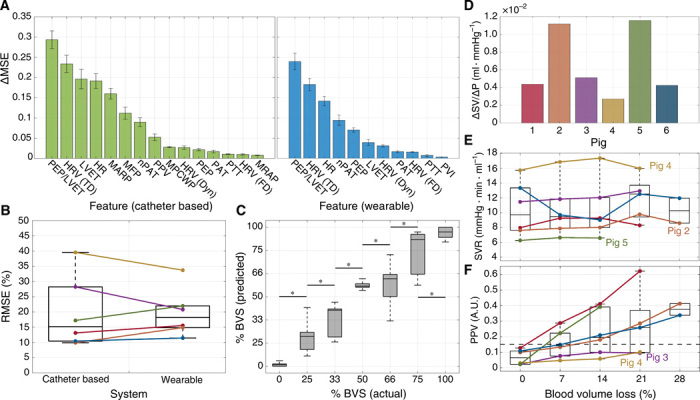
As the leading cause of trauma-related mortality, blood loss due to hemorrhage is notoriously difficult to triage and manage. To enable timely and appropriate care for patients with trauma, this work elucidates the externally measurable physiological features of exsanguination, which were used to develop a globalized model for assessing blood volume status (BVS) or the relative severity of blood loss. These features were captured via both a multimodal wearable system and a catheter-based reference and used to accurately infer BVS in a porcine model of hemorrhage (n = 6). Ultimately, high-level features of cardiomechanical function were shown to strongly predict progression toward cardiovascular collapse and used to estimate BVS with a median error of 15.17 and 18.17% for the catheter-based and wearable systems, respectively. Exploring the nexus of biomedical theory and practice, these findings lay the groundwork for digital biomarkers of hemorrhage severity and warrant further study in human subjects.
Copyright © 2020 The Authors, some rights reserved; exclusive licensee American Association for the Advancement of Science. No claim to original U.S. Government Works. Distributed under a Creative Commons Attribution License 4.0 (CC BY).
Figures
References
-
- Eastridge B. J., Hardin M., Cantrell J., Oetjen-Gerdes L., Zubko T., Mallak C., Wade C. E., Simmons J., Mace J., Mabry R., Bolenbaucher R., Blackbourne L. H., Died of wounds on the battlefield: Causation and implications for improving combat casualty care. J. Trauma 71, S4–S8 (2011). - PubMed
-
- Champion H. R., Bellamy R. F., Roberts C. P., Leppaniemi A., A profile of combat injury. J. Trauma 54, S13–S19 (2003). - PubMed
-
- Convertino V. A., Grudic G., Mulligan J., Moulton S., Estimation of individual-specific progression to impending cardiovascular instability using arterial waveforms. J. Appl. Physiol. 115, 1196–1202 (2013). - PubMed
-
- Acharya U. R., Joseph K. P., Kannathal N., Lim C. M., Suri J. S., Heart rate variability: A review. Med. Biol. Eng. Comput. 44, 1031–1051 (2006). - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
