

Improving Accuracy of Handoff by Implementing an Electronic Health Record-generated Tool: An Improvement Project in an Academic Neonatal Intensive Care Unit
- PMID: 32766500
- PMCID: PMC7360222
- DOI: 10.1097/pq9.0000000000000329
Improving Accuracy of Handoff by Implementing an Electronic Health Record-generated Tool: An Improvement Project in an Academic Neonatal Intensive Care Unit
Abstract
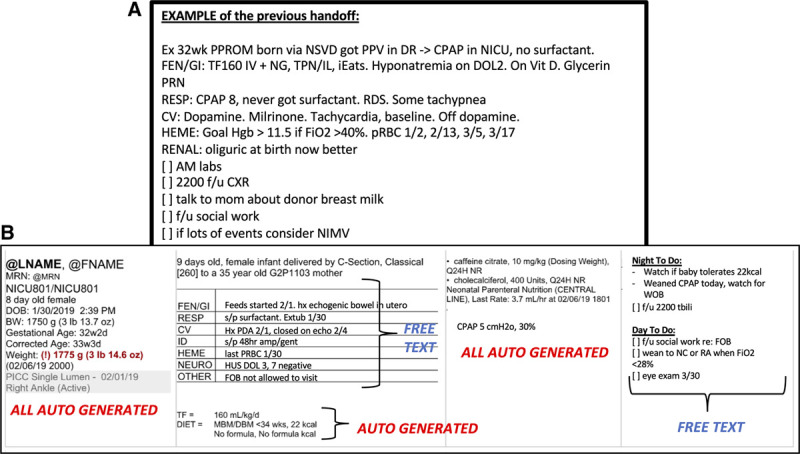
Background: Written patient handoffs are susceptible to errors or incompleteness. The accuracy is dependent on the person inputting the information. Thus, handoff printouts generated by electronic health records (EHR) with automation reduces the risk of transcription errors and improves consistency in format. This single-center quality improvement project aims to increase the accuracy of handoff printouts with an EHR-generated handoff tool.
Methods: This project used a plan-do-study-act methodology. Participants included registered nurses, neonatal nurse practitioners, neonatal hospitalists, pediatric residents, neonatal fellows, and neonatologists. The goals were to (1) increase accuracy of information to 80%, (2) reduce verbal handoff time by 20%, (3) reduce the frequency of incorrectly listed medications below 20%, and (4) improve user satisfaction by 1 point (on a 5-point Likert scale) over 6 months. Baseline assessment included a survey and a review of handoff reports 4 months before transitioning to the new handoff tool. We created a new handoff tool using EHR autogenerated phrases (Epic SmartPhrases) and autopopulated fields for pertinent Neonatal Intensive Care Unit patient data.
Results: After the unit-wide implementation of the new tool, the accuracy of 16 patient data points increased from 51% to 97%, while the frequency of patients with incorrectly listed medications decreased from 51% to 0%. Handoff time remained unchanged, while a 5-question user satisfaction survey showed an increase on the Likert scale.
Conclusions: We demonstrated that handoff printouts generated by EHR have fewer inaccuracies than manually scripted versions and do not add to the time required to give verbal handoff.
Copyright © 2020 the Author(s). Published by Wolters Kluwer Health, Inc.
Figures




References
-
- Devlin MK, Kozij NK, Kiss A, et al. Morning handover of on-call issues: opportunities for improvement. JAMA Intern Med. 2014;174:1479–1485. - PubMed
-
- Lin H, Lin E, Auditore S, et al. A narrative review of high-quality literature on the effects of resident duty hours reforms. Acad Med. 2016;91:140–150. - PubMed
-
- Rovner J. Accreditation council on graduate medical education (ACGME) Health Care Policy and Politics A to Z. 2009, Washington, DC: CQ Press; 12–12. doi: 10.4135/9781452240121.n6
-
- Samkoff JS, Jacques CH. A review of studies concerning effects of sleep deprivation and fatigue on residents’ performance. Acad Med. 1991;66:687–693. - PubMed
-
- Bell BM. Reconsideration of the New York state laws rationalizing the supervision and the working conditions of residents. Einstein J Biol Med. 2016;20:36.
LinkOut - more resources
Full Text Sources