

Preparedness and Reorganization of Care for Coronavirus Disease 2019 Patients in a Swiss ICU: Characteristics and Outcomes of 129 Patients
- PMID: 32766566
- PMCID: PMC7392615
- DOI: 10.1097/CCE.0000000000000173
Preparedness and Reorganization of Care for Coronavirus Disease 2019 Patients in a Swiss ICU: Characteristics and Outcomes of 129 Patients
Abstract
Objectives: In many countries, large numbers of critically ill patients with coronavirus disease 2019 are admitted to the ICUs within a short period of time, overwhelming usual care capacities. Preparedness and reorganization ahead of the wave to increase ICU surge capacity may be associated with favorable outcome. The purpose of this study was to report our experience in terms of ICU organization and anticipation, as well as reporting patient characteristics, treatment, and outcomes.
Design: A prospective observational study.
Setting: The division of intensive care at the Geneva University Hospitals (Geneva, Switzerland).
Patients: All consecutive adult patients with acute respiratory failure due to coronavirus disease 2019 admitted in the ICU between March 9, 2020, and May 19, 2020, were enrolled. Patients' demographic data, comorbidities, laboratory values, treatments, and clinical outcomes were collected.
Interventions: None.
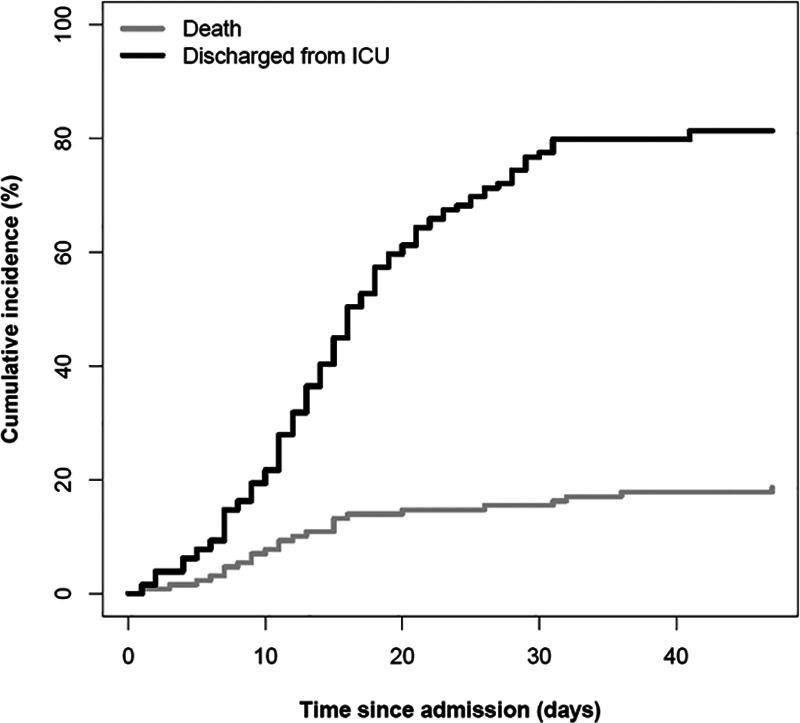
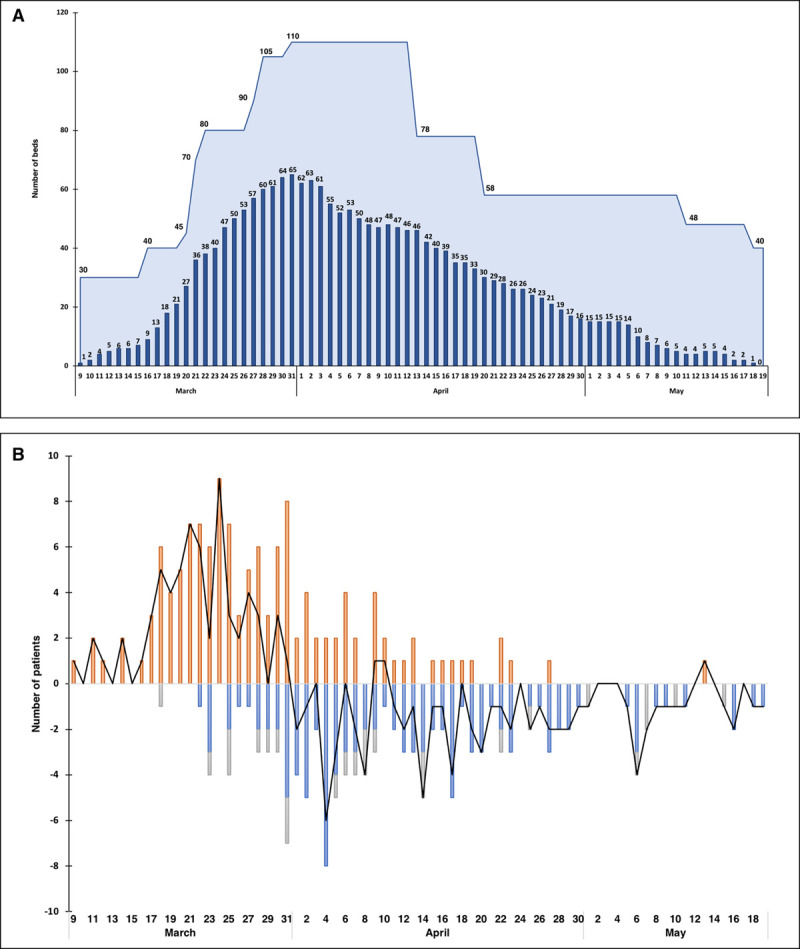
Measurements and main results: The ICU was reorganized into cells of six to eight patients under the care of three physicians and five nurses. Its capacity increased from 30 to 110 beds, fully equipped and staffed, transforming the surgical intermediate care unit, the postoperative care facility, and operating theaters into ICUs. Surge capacity has always exceeded the number of patients hospitalized. Among 129 critically ill patients with severe acute hypoxemic respiratory failure, 96% required invasive mechanical ventilation. A total of 105 patients (81%) were discharged alive and 24 died, corresponding to a mortality of 19%. Patients who died were significantly older, with higher severity scores at admission, had higher levels of d-dimers, plasma creatinine, high-sensitive troponin T, C-reactive protein, and procalcitonin, and required more frequent prone sessions.
Conclusions: A rapid increase in ICU bed capacity, including adequate equipment and staffing, allowed for a large number of critically ill coronavirus disease 2019 patients to be taken care of within a short period of time. Anticipation and preparedness ahead of the wave may account for the low mortality observed in our center. These results highlight the importance of resources management strategy in the context of the ongoing coronavirus disease 2019 pandemic.
Keywords: acute respiratory distress syndrome; coronavirus disease 2019; intensive care unit; mortality; severe acute respiratory syndrome coronavirus 2; surge capacity.
Copyright © 2020 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of the Society of Critical Care Medicine.
Conflict of interest statement
The authors have disclosed that they do not have any potential conflicts of interest.
Figures

References
-
- Pugin J. Le service de soins intensifs (réanimation) adultes à Genève, Suisse. Anesthésie & Réanimation. 2020; 6:182–187
-
- Swiss Federal Office of Public Health: COVID-19. Situation Suisse: Répartition par canton, âge et sexe. 2020 Available at: https://covid-19-schweiz.bagapps.ch/fr-1.html. Accessed April 22, 2020.
-
- Coronavirus Resource Center: COVID-19 Dashboard by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University (JHU). COVID-19 Map 2020, Baltimore, MD: Johns Hopkins University of Medicine; Available at: https://coronavirus.jhu.edu/map.html. Accessed April 22, 2020
-
- Swiss Federal Council: Le Conseil fédéral renforce les mesures contre le coronavirus pour protéger la santé de la population et soutient les secteurs touchés. 2020. Available at: https://www.admin.ch/gov/fr/accueil/documentation/communiques.msg-id-784.... Accessed April 22, 2020
LinkOut - more resources
Full Text Sources
Research Materials
