

Associations of Socioeconomic Status, Public vs Private Insurance, and Race/Ethnicity With Metastatic Sarcoma at Diagnosis
- PMID: 32766799
- PMCID: PMC7414392
- DOI: 10.1001/jamanetworkopen.2020.11087
Associations of Socioeconomic Status, Public vs Private Insurance, and Race/Ethnicity With Metastatic Sarcoma at Diagnosis
Abstract
Importance: Approximately 10% to 30% of patients with sarcoma present with detectable metastases at diagnosis. However, the extent to which presentation with metastases is due to delayed diagnosis vs other factors remains unclear.
Objective: To evaluate whether socioeconomic status, insurance status, or race/ethnicity were associated with the presence of metastases at diagnosis of sarcoma.
Design, setting, and participants: This cross-sectional study used data from the population-based Surveillance, Epidemiology, and End Results program. Adult and pediatric patients with an initial diagnosis of soft-tissue and bone sarcoma between 2001 and 2015 were stratified by age group (pediatric, <20 years; adult, 20-65 years; older adult, >65 years) and sarcoma subtype. Statistical analyses were performed between August 2019 and January 2020.
Exposures: Surveillance, Epidemiology, and End Results Census tract-level socioeconomic status index, insurance status, and race/ethnicity.
Main outcomes and measures: The odds of presenting with metastases at diagnosis were calculated.
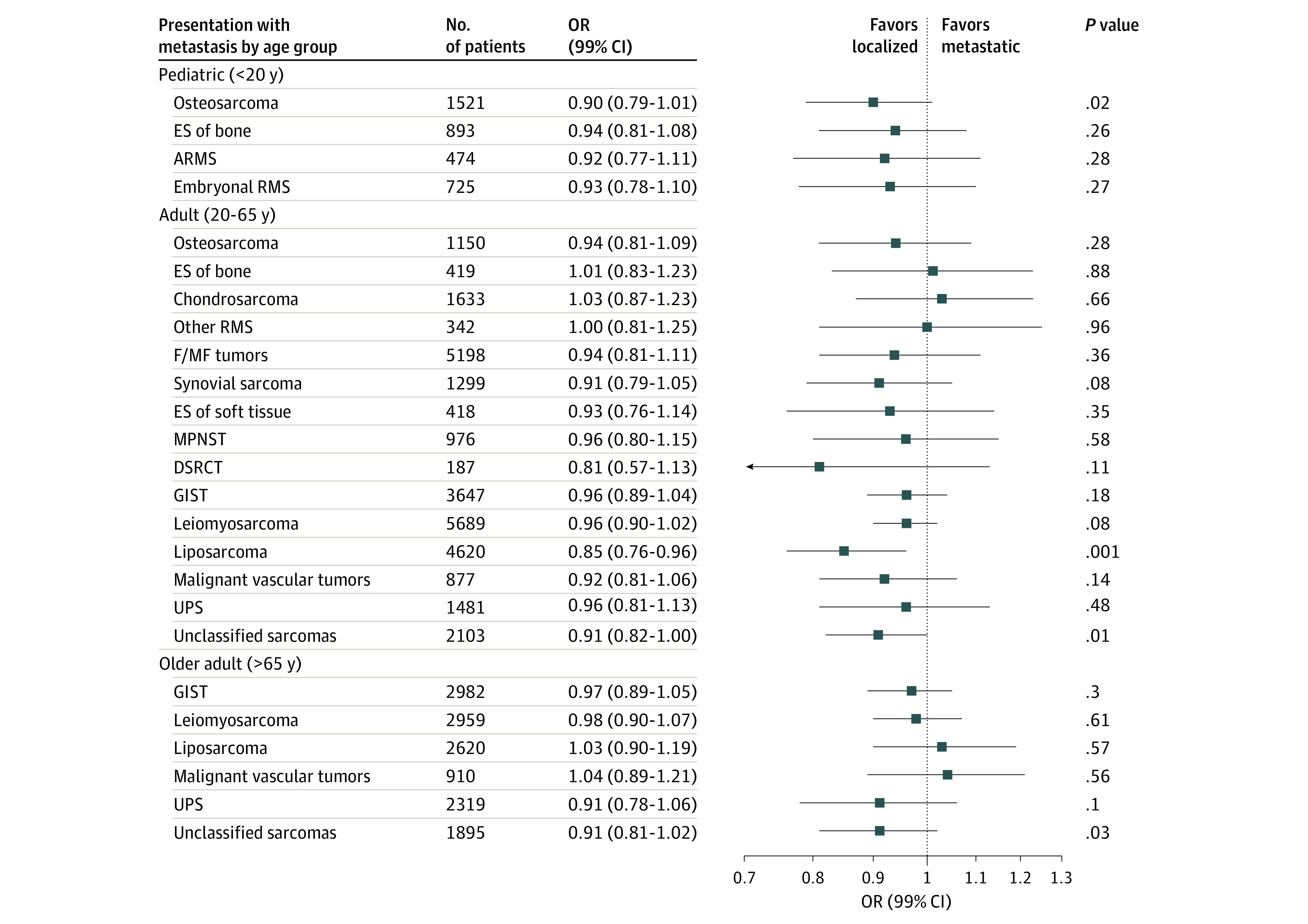
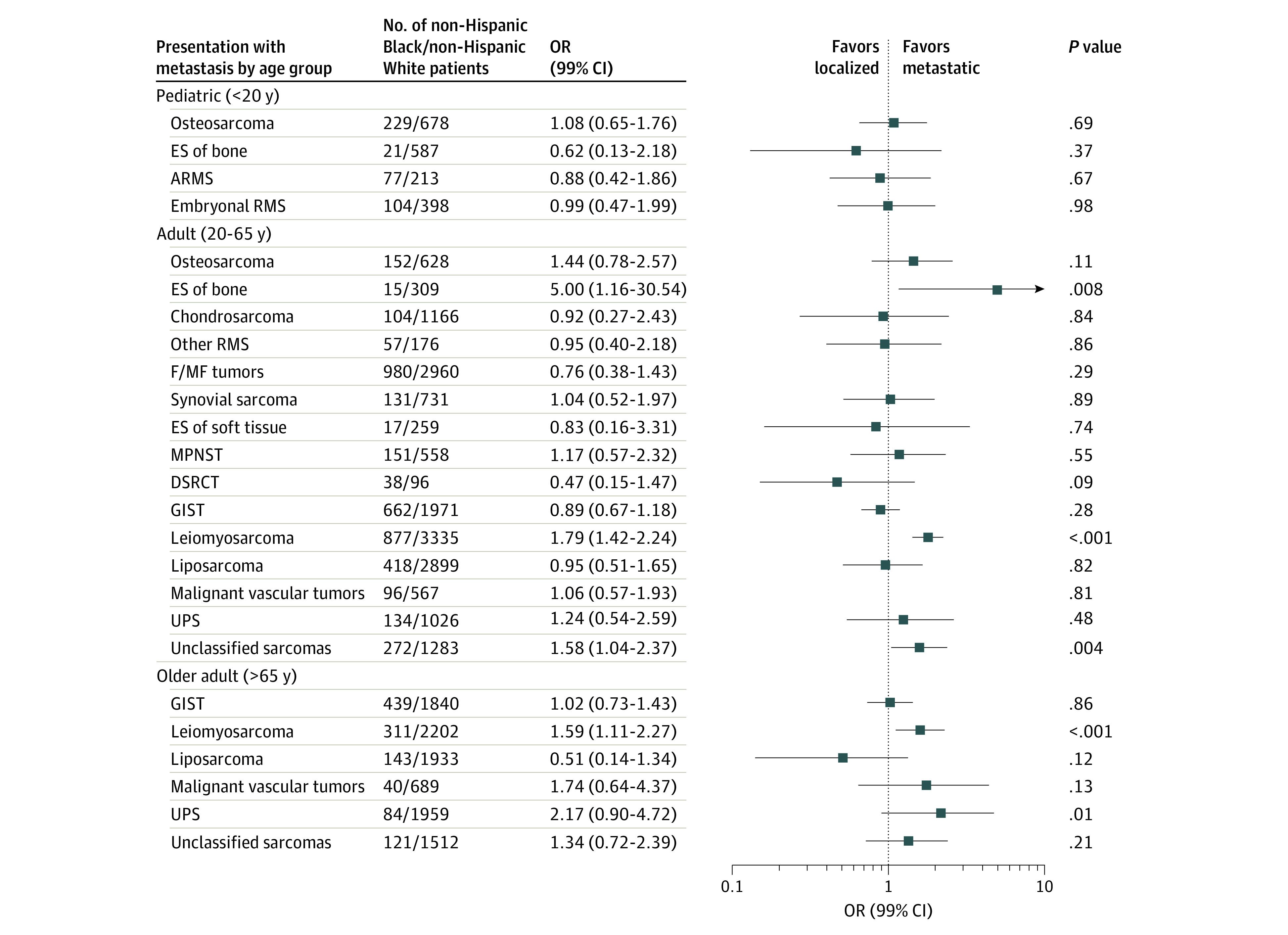
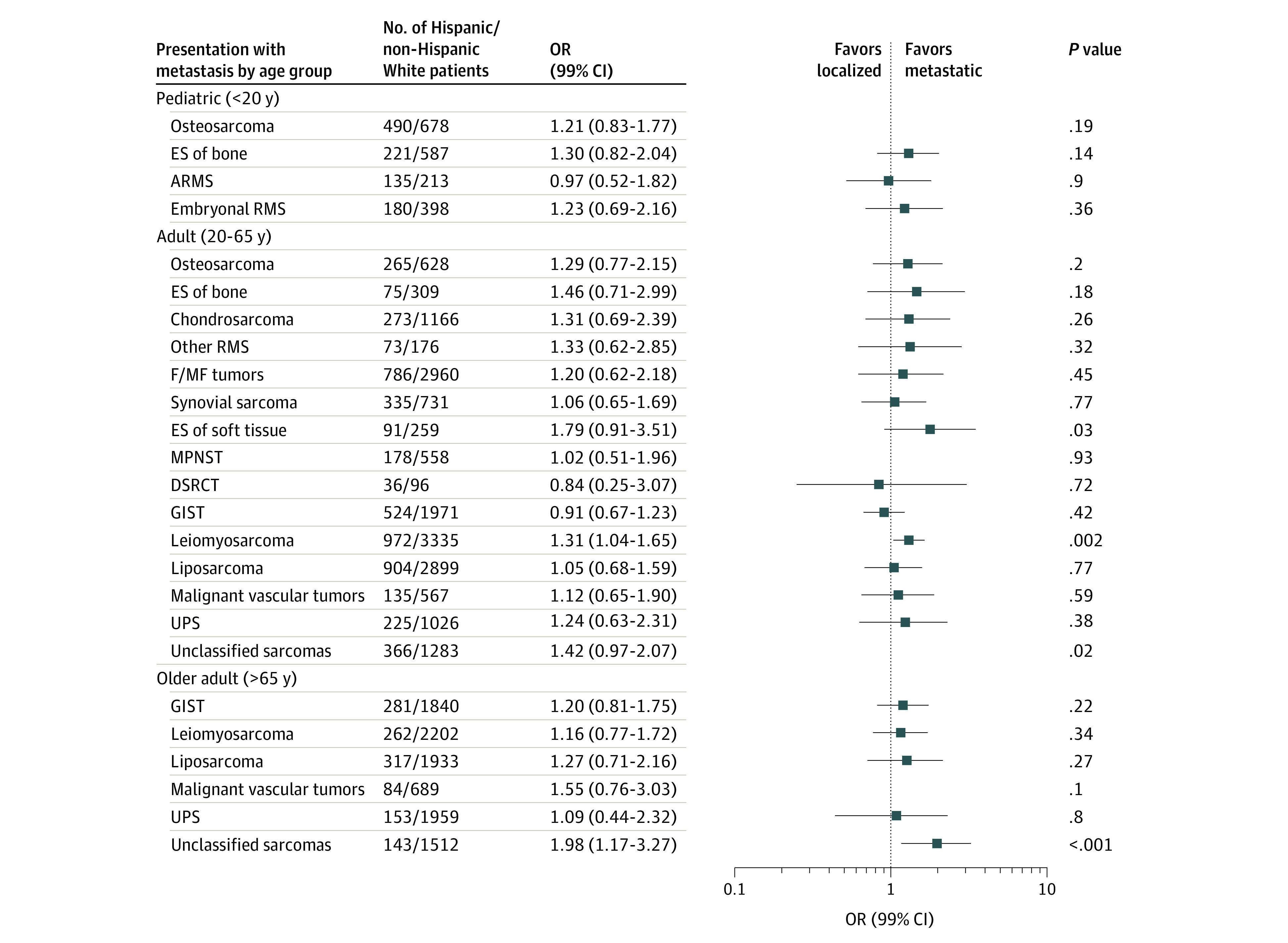
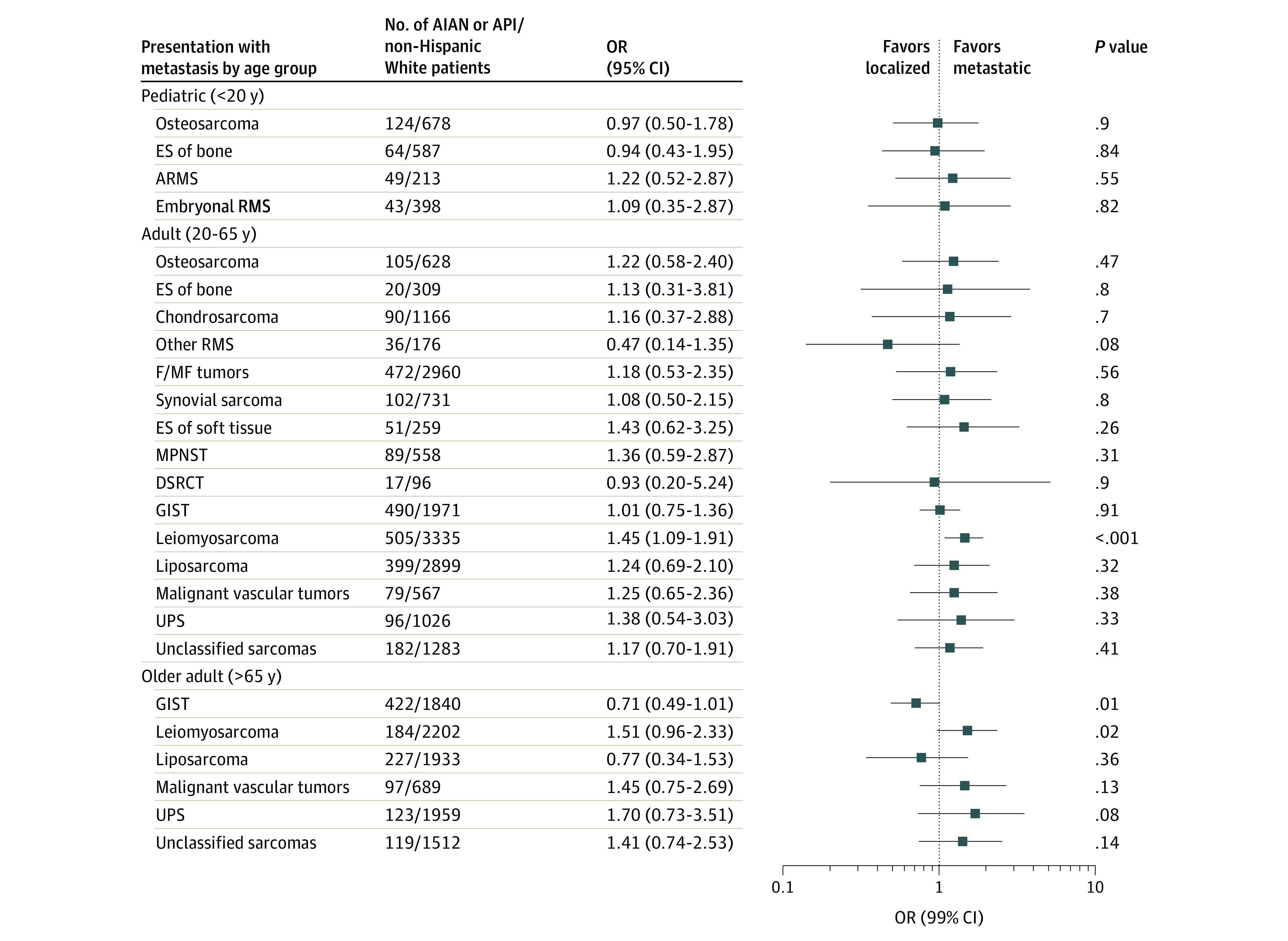
Results: A total of 47 337 patients with first primary malignant sarcoma were included (24 343 male patients [51.4%]), with 29 975 non-Hispanic White patients (63.3%), 5673 non-Hispanic Black patients (12.0%), 7504 Hispanic patients (15.8%), and 4185 American Indian-Alaskan Native and Asian Pacific Islander patients (8.8%). Liposarcoma in adults was the only subtype and age group combination that demonstrated a significant trend in incidence across socioeconomic status levels (odds ratio, 0.85; 99% CI, 0.76-0.96; P = .001). However, compared with having non-Medicaid insurance, having Medicaid or no insurance in adults was associated with an increased odds of metastases at diagnosis for 6 of the 8 sarcoma subtypes evaluated; osteosarcoma and Ewing sarcoma were the only 2 subtypes in adults for which metastases were not associated with insurance status. In addition, there was an increased risk of presenting with metastases among non-Hispanic Black adults diagnosed with leiomyosarcoma (odds ratio, 1.87; 99% CI, 1.41-2.48) and unclassified sarcomas (odds ratio, 1.65; 99% CI, 1.01-2.67) compared with non-Hispanic White adults that was independent of socioeconomic and insurance status.
Conclusions and relevance: These findings suggest that delayed access to care is associated with advanced stage at diagnosis for several soft-tissue sarcoma subtypes in adults, whereas other factors may be associated with the metastatic progression of osteosarcoma and Ewing sarcoma, as well as the racial disparities observed with metastatic leiomyosarcoma and unclassified sarcomas.
Conflict of interest statement
Figures
Similar articles
-
Association of Insurance Status and Racial Disparities With the Detection of Early-Stage Breast Cancer.JAMA Oncol. 2020 Mar 1;6(3):385-392. doi: 10.1001/jamaoncol.2019.5672. JAMA Oncol. 2020. PMID: 31917398 Free PMC article.
-
Is There an Association Between Insurance Status and Survival and Treatment of Primary Bone and Extremity Soft-tissue Sarcomas? A SEER Database Study.Clin Orthop Relat Res. 2020 Mar;478(3):527-536. doi: 10.1097/CORR.0000000000000889. Clin Orthop Relat Res. 2020. PMID: 31390340 Free PMC article.
-
Mediation of Racial and Ethnic Inequities in the Diagnosis of Advanced-Stage Cervical Cancer by Insurance Status.JAMA Netw Open. 2023 Mar 1;6(3):e232985. doi: 10.1001/jamanetworkopen.2023.2985. JAMA Netw Open. 2023. PMID: 36897588 Free PMC article.
-
Disparities in COVID-19 Outcomes by Race, Ethnicity, and Socioeconomic Status: A Systematic-Review and Meta-analysis.JAMA Netw Open. 2021 Nov 1;4(11):e2134147. doi: 10.1001/jamanetworkopen.2021.34147. JAMA Netw Open. 2021. PMID: 34762110 Free PMC article.
-
Demographic and socioeconomic disparities in pediatric cancer in the United States: Current knowledge, deepening understanding, and expanding intervention.Cancer Epidemiol. 2022 Feb;76:102082. doi: 10.1016/j.canep.2021.102082. Epub 2021 Dec 16. Cancer Epidemiol. 2022. PMID: 34923289 Review.
Cited by
-
No Geographical Inequalities in Survival for Sarcoma Patients in France: A Reference Networks' Outcome?Cancers (Basel). 2022 May 25;14(11):2620. doi: 10.3390/cancers14112620. Cancers (Basel). 2022. PMID: 35681600 Free PMC article.
-
Medicare Advantage in Soft Tissue Sarcoma May Be Associated with Worse Patient Outcomes.J Clin Med. 2023 Aug 4;12(15):5122. doi: 10.3390/jcm12155122. J Clin Med. 2023. PMID: 37568523 Free PMC article.
-
Supporting Participant Engagement in Cancer Genomics Research in Rare Cancers: A Qualitative Study of Patients, Caregivers, and Advocates.Cancer Control. 2025 Jan-Dec;32:10732748251364041. doi: 10.1177/10732748251364041. Epub 2025 Jul 28. Cancer Control. 2025. PMID: 40719570 Free PMC article.
-
Odds of Metastatic Disease at Diagnosis of Primary Bone and Soft-Tissue Sarcomas of the Extremity and Pelvis Based on Preferred Language and Socioeconomic Factors.J Am Acad Orthop Surg. 2025 Mar 15;33(6):319-326. doi: 10.5435/JAAOS-D-24-00634. Epub 2024 Dec 27. J Am Acad Orthop Surg. 2025. PMID: 39729593 Free PMC article.
-
Tumor grade and symptoms at presentation are survival risk factors in Chinese patients with primary retroperitoneal sarcoma.J Clin Transl Res. 2022 Nov 24;8(6):584-593. eCollection 2022 Dec 29. J Clin Transl Res. 2022. PMID: 36683651 Free PMC article.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
