

Multiplatform molecular test performance in indeterminate thyroid nodules
- PMID: 32767735
- PMCID: PMC7754490
- DOI: 10.1002/dc.24564
Multiplatform molecular test performance in indeterminate thyroid nodules
Abstract
Background: Approximately 25% of thyroid nodule fine-needle aspirates (FNAs) have cytology that is indeterminate for malignant disease. Accurate risk stratification of these FNAs with ancillary testing would reduce unnecessary thyroid surgery.
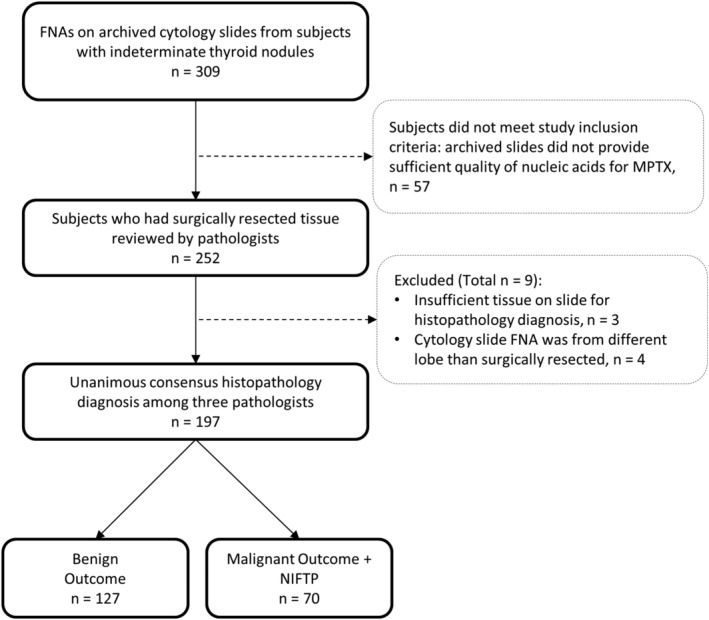
Methods: We evaluated the performance of an ancillary multiplatform test (MPTX) that has three diagnostic categories (negative, moderate, and positive). MPTX includes the combination of a mutation panel (ThyGeNEXT®) and a microRNA risk classifier (ThyraMIR®). A blinded, multicenter study was performed using consensus histopathology diagnosis among three pathologists to validate test performance.
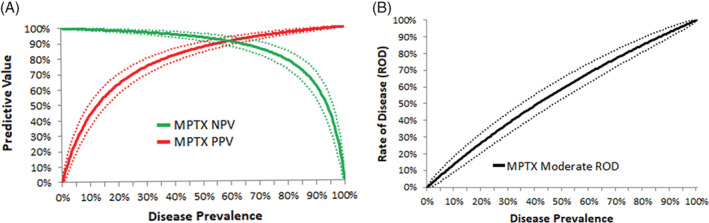
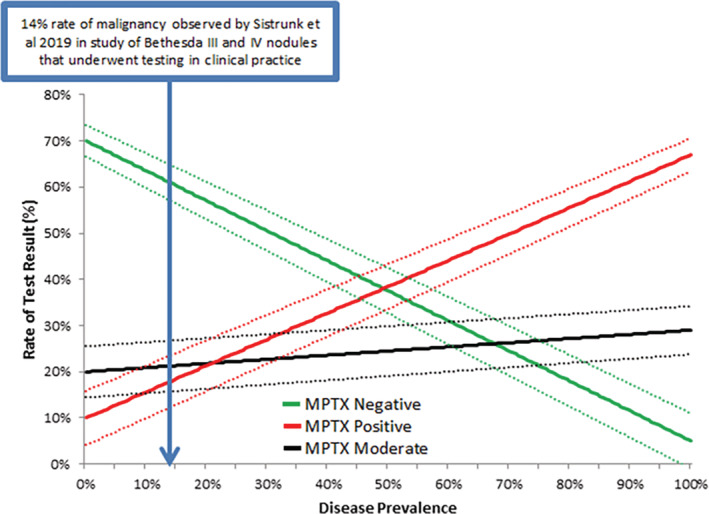
Results: Unanimous consensus diagnosis was reached in 197 subjects with indeterminate thyroid nodules; 36% had disease. MPTX had 95% sensitivity (95% CI,86%-99%) and 90% specificity (95% CI,84%-95%) for disease in prevalence adjusted nodules with Bethesda III and IV cytology. Negative MPTX results ruledout disease with 97% negative predictive value (NPV; 95% CI,91%-99%) at a 30% disease prevalence, while positive MPTX results ruledin high risk disease with 75% positive predictive value (PPV; 95% CI,60%-86%). Such results are expected in four out of five Bethesda III and IV nodules tested, including RAS positive nodules in which the microRNA classifier was useful in rulingin disease. 90% of mutation panel false positives were due to analytically verified RAS mutations detected in benign adenomas. Moderate MPTX results had a moderate rate of disease (39%, 95% CI,23%-54%), primarily due to RAS mutations, wherein the possibility of disease could not be excluded.
Conclusions: Our results emphasize that decisions for surgery should not solely be based on RAS or RAS-like mutations. MPTX informs management decisions while accounting for these challenges.
Keywords: indeterminate thyroid nodules; malignancy; molecular test; outcomes.
© 2020 The Authors. Diagnostic Cytopathology published by Wiley Periodicals LLC.
Conflict of interest statement
J. Woody Sistrunk, Nicole Massoll, Ryan Campbell, Ann E. Walts, and Shikha Bose received institutional research funding from Interpace Diagnostics. Mark A. Lupo has received research funding from Interpace Diagnostics. J. Woody Sistrunk and Nicole Massoll are consultants for Interpace Diagnostics. Histopathology review by Thomas J. Giordano and Peter M. Sadow was funded by Interpace Diagnostics. Sara A. Jackson, Christina M. Narick, Nicole Toney, Sydney D. Finkelstein, Alidad Mireskandari, Gyanendra Kumar are employees of Interpace Diagnostics.
Figures
References
-
- Howlader NNA, Krapcho M, Miller D, et al., eds. SEER Cancer Statistics Review, 1975–2017. Bethesda, MD: National Cancer Institute; 2020. https://seer.cancer.gov/csr/1975_2017/, based on November 2019 SEER data submission, posted to the SEER web site, April 2020.
-
- Cibas ES, Ali SZ. The 2017 Bethesda system for reporting thyroid cytopathology. Thyroid. 2017;27(11):1341‐1346. - PubMed
-
- Ablordeppey KK, Timmaraju VA, Song‐Yang JW, et al. Development and analytical validation of an expanded mutation detection panel for next‐generation sequencing of thyroid nodule aspirates. J Mol Diagn. 2020;22(3):355‐367. - PubMed
