

The efficacy and safety of oral paracetamol versus oral ibuprofen for patent ductus arteriosus closure in preterm neonates - A systematic review and meta-analysis
- PMID: 32768013
- PMCID: PMC7411098
- DOI: 10.1016/j.ihj.2020.05.012
The efficacy and safety of oral paracetamol versus oral ibuprofen for patent ductus arteriosus closure in preterm neonates - A systematic review and meta-analysis
Abstract
Objective: This systematic review and meta-analysis aimed to synthesize the latest evidence on the efficacy and safety of oral acetaminophen compared to oral ibuprofen for patent ductus arteriosus (PDA) in preterm infants.
Methods: We performed a systematic literature search on topics that assesses the use of oral paracetamol compared to oral ibuprofen in preterm neonates diagnosed with PDA from PubMed, EuropePMC, Cochrane Central Database, ScienceDirect, ProQuest, ClinicalTrials.gov, and hand-sampling from potential articles.
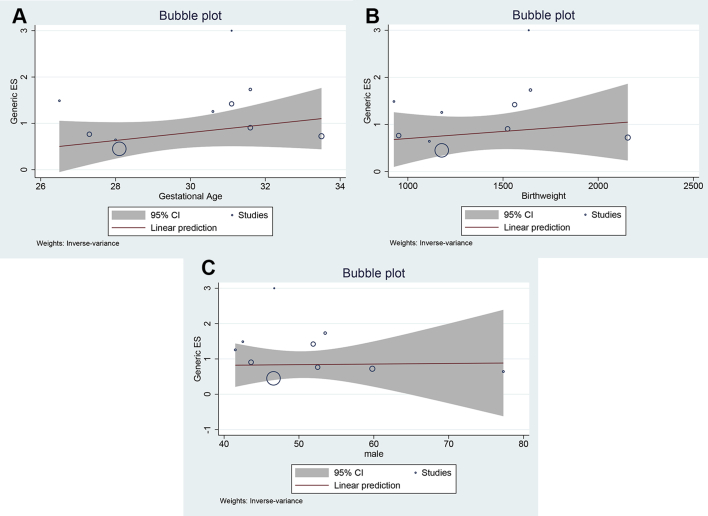
Results: There were 1547 subjects from 10 selected studies. Primary closure rate was similar in both groups. Subgroup analysis on studies enrolling neonates with ≤30 weeks gestational age showed that ibuprofen was superior (OR 0.52 [0.31, 0.90], I2: 0%). On the other hand, paracetamol was superior neonates with ≤34 weeks gestational age (OR 1.73 [1.01, 2.94], I2: 30%). Reopening rate, surgical closure rate, mortality, intraventricular hemorrhage, and necrotizing enterocolitis were similar in both groups. Rate of renal dysfunction (OR 0.27 [0.10, 0.77], I2: 0%) and gastrointestinal bleeding (OR 0.31 [0.11, 0.88], I2: 0%) were lower in paracetamol group. Subgroup analysis of randomized controlled studies (RCTs) showed similar results. Meta-regression analysis showed that the primary closure rate was not influenced by gestational age, birth weight, and gender. GRADE demonstrates a low level of certainty for primary closure and mortality. Renal dysfunction and gastrointestinal bleeding havea moderate level of certainty.
Conclusion: There was no significant difference between the efficacy of oral paracetamol and oral ibuprofen. However, the rate of renal dysfunction and gastrointestinal bleeding were higher in oral ibuprofen.
Keywords: Ibuprofen; Neonate; Paracetamol; Patent ductus arteriosus; Preterm.
Copyright © 2020 Cardiological Society of India. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Competing interests statement All authors have none to declare.
Figures



References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
