

Adherence to Healthy Dietary Patterns and Risk of CKD Progression and All-Cause Mortality: Findings From the CRIC (Chronic Renal Insufficiency Cohort) Study
- PMID: 32768632
- PMCID: PMC7855760
- DOI: 10.1053/j.ajkd.2020.04.019
Adherence to Healthy Dietary Patterns and Risk of CKD Progression and All-Cause Mortality: Findings From the CRIC (Chronic Renal Insufficiency Cohort) Study
Abstract
Rationale & objective: Current dietary guidelines recommend that patients with chronic kidney disease (CKD) restrict individual nutrients, such as sodium, potassium, phosphorus, and protein. This approach can be difficult for patients to implement and ignores important nutrient interactions. Dietary patterns are an alternative method to intervene on diet. Our objective was to define the associations of 4 healthy dietary patterns with risk for CKD progression and all-cause mortality among people with CKD.
Study design: Prospective cohort study.
Setting & participants: 2,403 participants aged 21 to 74 years with estimated glomerular filtration rates of 20 to 70mL/min/1.73m2 and dietary data in the Chronic Renal Insufficiency Cohort (CRIC) Study.
Exposures: Healthy Eating Index-2015, Alternative Healthy Eating Index-2010, alternate Mediterranean diet (aMed), and Dietary Approaches to Stop Hypertension (DASH) diet scores were calculated from food frequency questionnaires.
Outcomes: (1) CKD progression defined as≥50% estimated glomerular filtration rate decline, kidney transplantation, or dialysis and (2) all-cause mortality.
Analytical approach: Cox proportional hazards regression models adjusted for demographic, lifestyle, and clinical covariates to estimate hazard ratios (HRs) and 95% CIs.
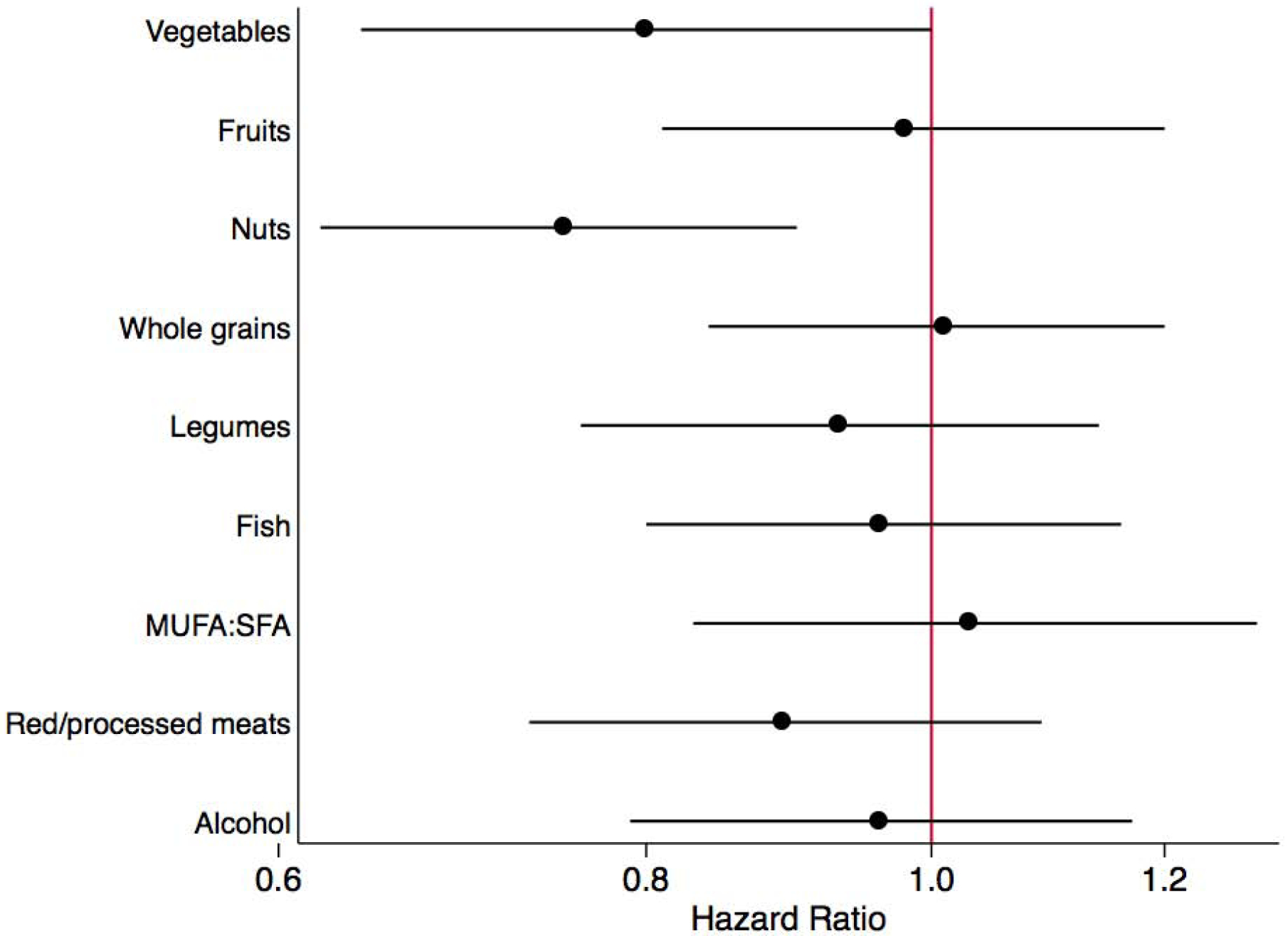
Results: There were 855 cases of CKD progression and 773 deaths during a maximum of 14 years. Compared with participants with the lowest adherence, the most highly adherent tertile of Alternative Healthy Eating Index-2010, aMed, and DASH had lower adjusted risk for CKD progression, with the strongest results for aMed (HR, 0.75; 95% CI, 0.62-0.90). Compared with participants with the lowest adherence, the highest adherence tertiles for all scores had lower adjusted risk for all-cause mortality for each index (24%-31% lower risk).
Limitations: Self-reported dietary intake.
Conclusions: Greater adherence to several healthy dietary patterns is associated with lower risk for CKD progression and all-cause mortality among people with CKD. Guidance to adopt healthy dietary patterns can be considered as a strategy for managing CKD.
Keywords: CKD progression; Dietary patterns; chronic kidney disease (CKD); dietary intake; dietary score; food frequency questionnaire (FFQ); healthy eating; modifiable risk factor; mortality; nutrition; renal.
Copyright © 2020 National Kidney Foundation, Inc. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Financial Disclosure: Dr. Scialla has received consulting fees from Tricida and modest research support for clinical trial event committees from GlaxoSmithKline and Sanofi. The remaining authors declare that they have no other relevant financial interests.
Figures
References
-
- Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med. 2004;351(13):1296–305. - PubMed
Publication types
MeSH terms
Grants and funding
- UL1 TR002548/TR/NCATS NIH HHS/United States
- R21 HL143089/HL/NHLBI NIH HHS/United States
- T32 HL007024/HL/NHLBI NIH HHS/United States
- UL1 RR024131/RR/NCRR NIH HHS/United States
- U01 DK061022/DK/NIDDK NIH HHS/United States
- UL1 TR000439/TR/NCATS NIH HHS/United States
- U01 DK060990/DK/NIDDK NIH HHS/United States
- UL1 RR029879/RR/NCRR NIH HHS/United States
- U01 DK061028/DK/NIDDK NIH HHS/United States
- UL1 TR000433/TR/NCATS NIH HHS/United States
- K24 DK092290/DK/NIDDK NIH HHS/United States
- R01 DK072231/DK/NIDDK NIH HHS/United States
- U01 DK060984/DK/NIDDK NIH HHS/United States
- U01 DK061021/DK/NIDDK NIH HHS/United States
- U24 DK060990/DK/NIDDK NIH HHS/United States
- K01 DK107782/DK/NIDDK NIH HHS/United States
- U01 DK060980/DK/NIDDK NIH HHS/United States
- UC4 DK101108/DK/NIDDK NIH HHS/United States
- R01 HL127028/HL/NHLBI NIH HHS/United States
- U01 DK060963/DK/NIDDK NIH HHS/United States
- P30 DK072488/DK/NIDDK NIH HHS/United States
- UL1 TR000003/TR/NCATS NIH HHS/United States
- UL1 TR000424/TR/NCATS NIH HHS/United States
- M01 RR016500/RR/NCRR NIH HHS/United States
- P20 GM109036/GM/NIGMS NIH HHS/United States
- U01 DK060902/DK/NIDDK NIH HHS/United States
- K23 DK094829/DK/NIDDK NIH HHS/United States
- K24 HL148181/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
