

Thyroid cancer diagnosis by Raman spectroscopy
- PMID: 32770073
- PMCID: PMC7414870
- DOI: 10.1038/s41598-020-70165-0
Thyroid cancer diagnosis by Raman spectroscopy
Abstract
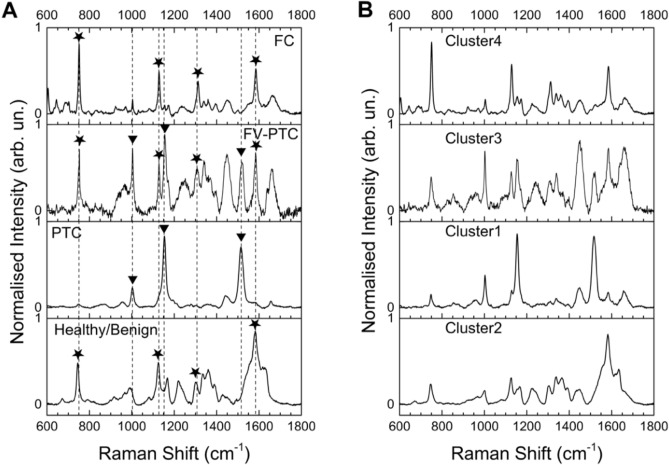
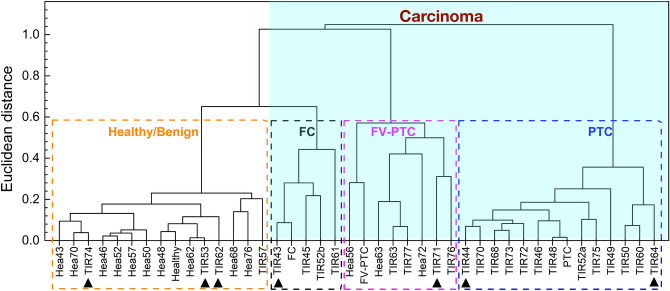
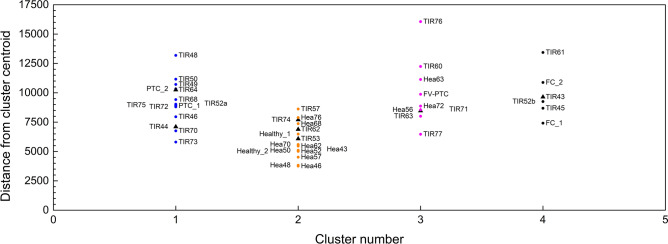
Over the last 50 years, the incidence of human thyroid cancer disease has seen a significative increment. This comes along with an even higher increment of surgery, since, according to the international guidelines, patients are sometimes addressed to surgery also when the fine needle aspiration gives undetermined cytological diagnosis. As a matter of fact, only 30% of the thyroid glands removed for diagnostic purpose have a post surgical histological report of malignancy: this implies that about 70% of the patients have suffered an unnecessary thyroid removal. Here we show that Raman spectroscopy investigation of thyroid tissues provides reliable cancer diagnosis. Healthy tissues are consistently distinguished from cancerous ones with an accuracy of [Formula: see text] 90%, and the three cancer typology with highest incidence are clearly identified. More importantly, Raman investigation has evidenced alterations suggesting an early stage of transition of adenoma tissues into cancerous ones. These results suggest that Raman spectroscopy may overcome the limits of current diagnostic tools.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
