

Mortality in adults with multidrug-resistant tuberculosis and HIV by antiretroviral therapy and tuberculosis drug use: an individual patient data meta-analysis
- PMID: 32771107
- PMCID: PMC8094110
- DOI: 10.1016/S0140-6736(20)31316-7
Mortality in adults with multidrug-resistant tuberculosis and HIV by antiretroviral therapy and tuberculosis drug use: an individual patient data meta-analysis
Erratum in
-
Department of Error.Lancet. 2020 Sep 26;396(10255):886. doi: 10.1016/S0140-6736(20)31971-1. Lancet. 2020. PMID: 32979976 No abstract available.
Abstract
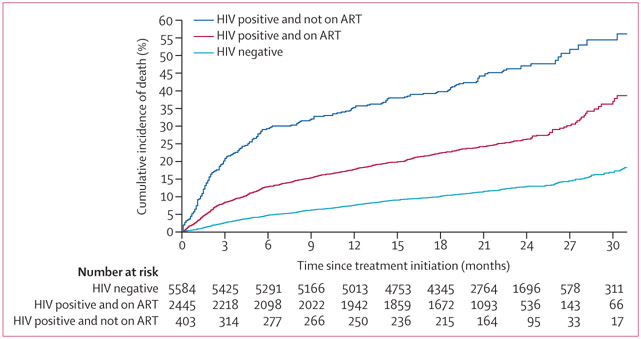
Background: HIV-infection is associated with increased mortality during multidrug-resistant tuberculosis treatment, but the extent to which the use of antiretroviral therapy (ART) and anti-tuberculosis medications modify this risk are unclear. Our objective was to evaluate how use of these treatments altered mortality risk in HIV-positive adults with multidrug-resistant tuberculosis.
Methods: We did an individual patient data meta-analysis of adults 18 years or older with confirmed or presumed multidrug-resistant tuberculosis initiating tuberculosis treatment between 1993 and 2016. Data included ART use and anti-tuberculosis medications grouped according to WHO effectiveness categories. The primary analysis compared HIV-positive with HIV-negative patients in terms of death during multidrug-resistant tuberculosis treatment, excluding those lost to follow up, and was stratified by ART use. Analyses used logistic regression after exact matching on country World Bank income classification and drug resistance and propensity-score matching on age, sex, geographic site, year of multidrug-resistant tuberculosis treatment initiation, previous tuberculosis treatment, directly observed therapy, and acid-fast-bacilli smear-positivity to obtain adjusted odds ratios (aORs) and 95% CIs. Secondary analyses were conducted among those with HIV-infection.
Findings: We included 11 920 multidrug-resistant tuberculosis patients. 2997 (25%) were HIV-positive and on ART, 886 (7%) were HIV-positive and not on ART, and 1749 (15%) had extensively drug-resistant tuberculosis. By use of HIV-negative patients as reference, the aOR of death was 2·4 (95% CI 2·0-2·9) for all patients with HIV-infection, 1·8 (1·5-2·2) for HIV-positive patients on ART, and 4·2 (3·0-5·9) for HIV-positive patients with no or unknown ART. Among patients with HIV, use of at least one WHO Group A drug and specific use of moxifloxacin, levofloxacin, bedaquiline, or linezolid were associated with significantly decreased odds of death.
Interpretation: Use of ART and more effective anti-tuberculosis drugs is associated with lower odds of death among HIV-positive patients with multidrug-resistant tuberculosis. Access to these therapies should be urgently pursued.
Funding: American Thoracic Society, Canadian Institutes of Health Research, US Centers for Disease Control and Prevention, European Respiratory Society, Infectious Diseases Society of America.
Copyright © 2020 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests
CL reports personal fees from Chiesi, Gilead, Janssen, Lucane, Novartis, Thermofisher, Oxford Immunotec, and Transgene, outside the submitted work. All other authors declare no competing interests.
Figures
Comment in
-
Optimal therapy for multidrug-resistant tuberculosis and HIV.Lancet. 2020 Aug 8;396(10248):363-365. doi: 10.1016/S0140-6736(20)31688-3. Lancet. 2020. PMID: 32771093 No abstract available.
References
-
- WHO. Global tuberculosis report 2019. Geneva: World Health Organization, 2019.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
