

Fine-Needle Aspiration-Based Patient-Derived Cancer Organoids
- PMID: 32771978
- PMCID: PMC7415927
- DOI: 10.1016/j.isci.2020.101408
Fine-Needle Aspiration-Based Patient-Derived Cancer Organoids
Abstract
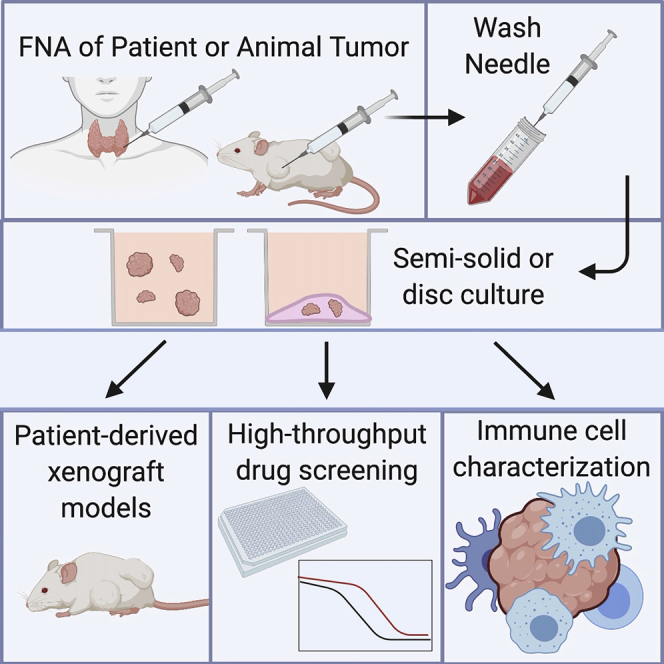
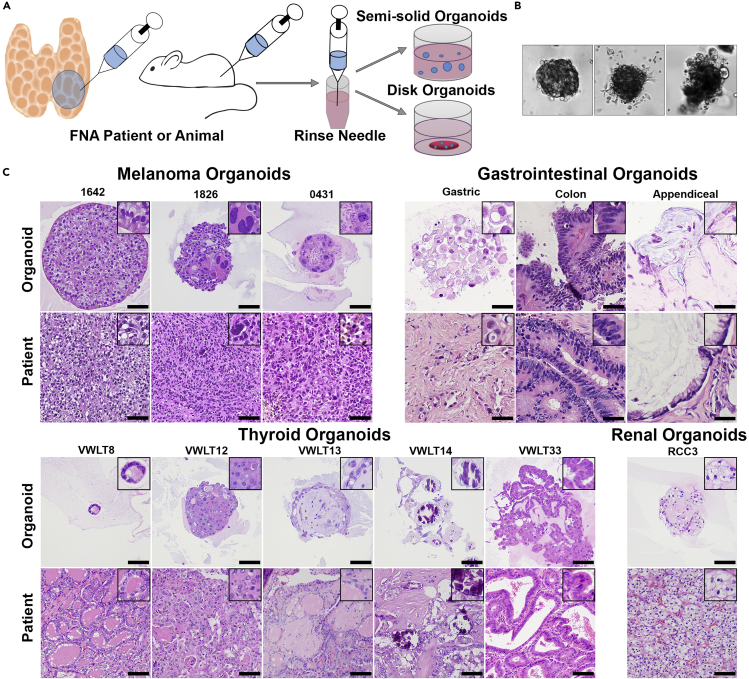
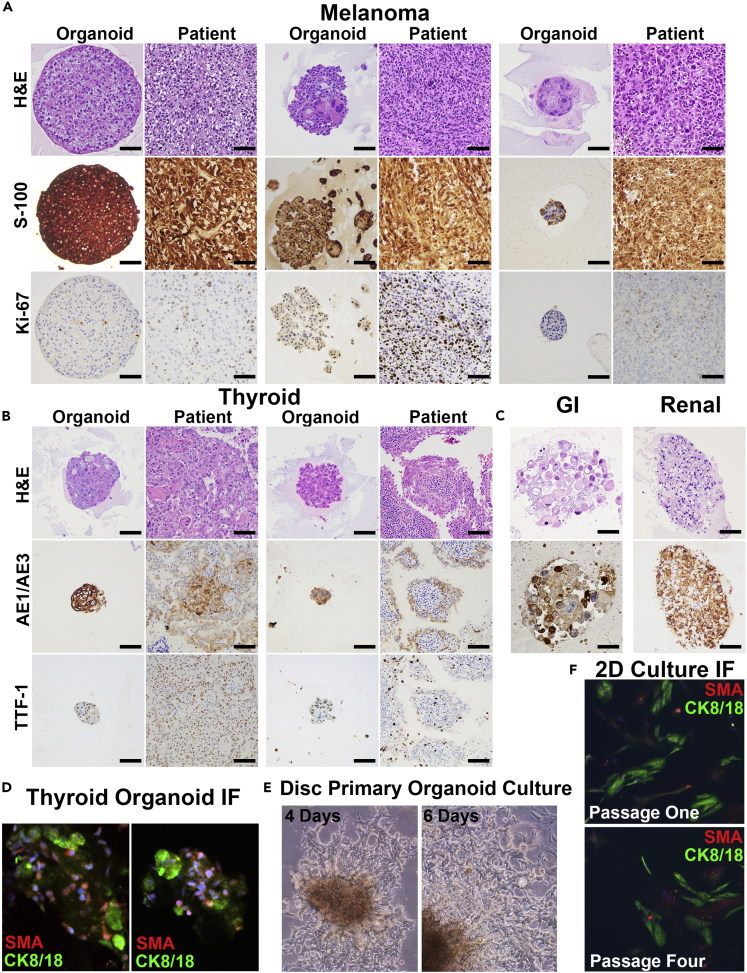
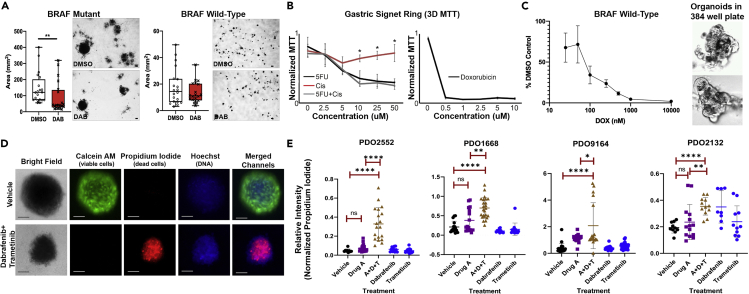
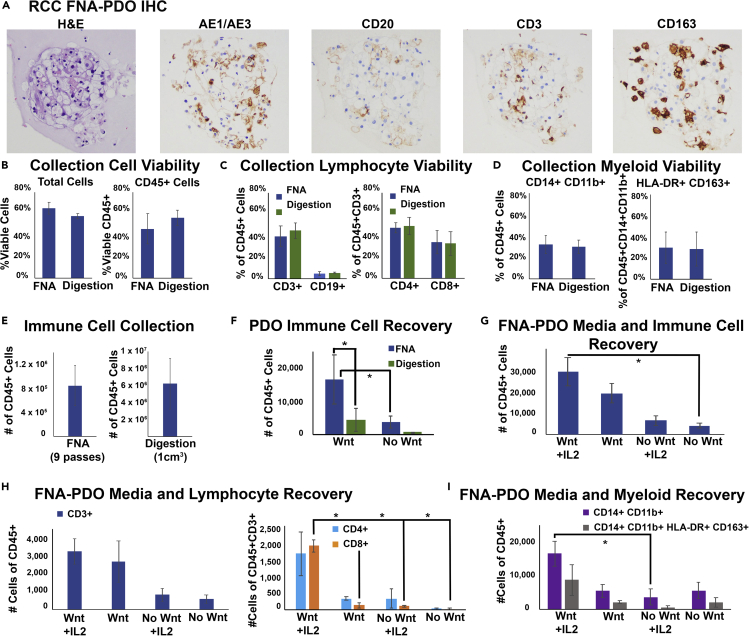
Patient-derived cancer organoids hold great potential to accurately model and predict therapeutic responses. Efficient organoid isolation methods that minimize post-collection manipulation of tissues would improve adaptability, accuracy, and applicability to both experimental and real-time clinical settings. Here we present a simple and minimally invasive fine-needle aspiration (FNA)-based organoid culture technique using a variety of tumor types including gastrointestinal, thyroid, melanoma, and kidney. This method isolates organoids directly from patients at the bedside or from resected tissues, requiring minimal tissue processing while preserving the histologic growth patterns and infiltrating immune cells. Finally, we illustrate diverse downstream applications of this technique including in vitro high-throughput chemotherapeutic screens, in situ immune cell characterization, and in vivo patient-derived xenografts. Thus, routine clinical FNA-based collection techniques represent an unappreciated substantial source of material that can be exploited to generate tumor organoids from a variety of tumor types for both discovery and clinical applications.
Keywords: Cancer; Clinical Medicine; Tissue Engineering.
Copyright © 2020 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of Interests The authors declare no competing interests.
Figures
References
-
- Austin R.M., Birdsong G.G., Sidawy M.K., Kaminsky D.B. Fine needle aspiration is a feasible and accurate technique in the diagnosis of lymphoma. J. Clin. Oncol. 2005;23:9029–9030. author reply 9030-9021. - PubMed
-
- Baatenburg de Jong R.J., Rongen R.J., Verwoerd C.D., van Overhagen H., Lameris J.S., Knegt P. Ultrasound-guided fine-needle aspiration biopsy of neck nodes. Arch. Otolaryngol. Head Neck Surg. 1991;117:402–404. - PubMed
-
- Bar-Ephraim Y.E., Kretzschmar K., Clevers H. Organoids in immunological research. Nat. Rev. Immunol. 2019;20:279–293. - PubMed
-
- Boyd J.D., Smith G.D., Hong H., Mageau R., Juskevicius R. Fine-needle aspiration is superior to needle core biopsy as a sample acquisition method for flow cytometric analysis in suspected hematologic neoplasms. Cytometry B Clin. Cytom. 2015;88:64–68. - PubMed
Grants and funding
- I01 BX002301/BX/BLRD VA/United States
- S10 OD023475/OD/NIH HHS/United States
- K12 CA090625/CA/NCI NIH HHS/United States
- K08 CA240901/CA/NCI NIH HHS/United States
- P30 DK058404/DK/NIDDK NIH HHS/United States
- R01 CA243326/CA/NCI NIH HHS/United States
- R35 GM122516/GM/NIGMS NIH HHS/United States
- T32 GM007347/GM/NIGMS NIH HHS/United States
- P30 CA068485/CA/NCI NIH HHS/United States
- T32 GM152284/GM/NIGMS NIH HHS/United States
- R01 CA116021/CA/NCI NIH HHS/United States
- R37 CA233770/CA/NCI NIH HHS/United States
- R01 CA244188/CA/NCI NIH HHS/United States
- U24 DK059637/DK/NIDDK NIH HHS/United States
- T32 GM007628/GM/NIGMS NIH HHS/United States
- R01 CA222594/CA/NCI NIH HHS/United States
- IK6 BX005225/BX/BLRD VA/United States
- R01 CA203012/CA/NCI NIH HHS/United States
- R50 CA211206/CA/NCI NIH HHS/United States
- R01 CA217987/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
