

Management of Aortic Stenosis in Patients With End-Stage Renal Disease on Hemodialysis
- PMID: 32772570
- PMCID: PMC7422925
- DOI: 10.1161/CIRCINTERVENTIONS.120.009252
Management of Aortic Stenosis in Patients With End-Stage Renal Disease on Hemodialysis
Abstract
Background: Patients with end-stage renal disease on hemodialysis (ESRD-HD) and aortic stenosis have poor prognosis. The role of transcatheter aortic valve replacement (TAVR) in this high-risk population is debated.
Methods: We compared the outcomes among ESRD-HD Medicare beneficiaries who were managed with TAVR, surgical AVR (SAVR), or conservative management for aortic stenosis between 2015 and 2017, using overlap propensity score weighting analysis to control for differences in treatment assignment. The primary outcome was all-cause mortality and was compared between treatment groups as well as to age-sex matched mortality for ESRD-HD in the US population. Secondary outcomes included trend of heart failure hospitalizations.
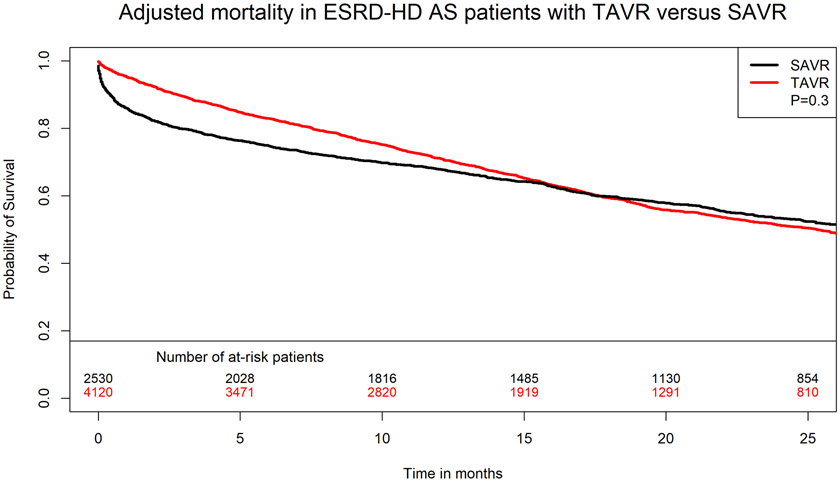
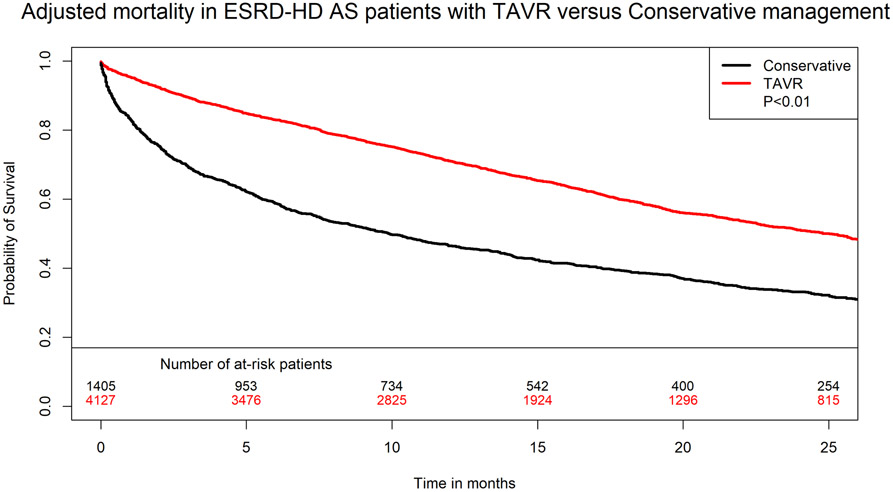
Results: A total of 8107 ESRD-HD patients with aortic stenosis were included, 4130 (50%) underwent TAVR, 2565 (31.6%) underwent SAVR, and 1412 (17.4%) were managed conservatively. TAVR patients had more comorbidities and higher frailty compared with the other 2 groups. Thirty-day mortality was lower with TAVR compared with SAVR (4.6% versus 12.8%, P<0.01). After a median follow-up of 465 days (interquartile range, 261-759), on overlap propensity score weighting analysis, there was no difference in mortality between TAVR and SAVR (adjusted hazard ratio, 1.02 [95% CI, 0.91-1.15], P=0.7), and mortality was lower with TAVR compared with conservative management (adjusted hazard ratio, 0.53 [95% CI, 0.47-0.60], P<0.001). Standardized mortality ratios with TAVR, SAVR, and conservative management compared with age-sex matched ESRD-HD US population were 1.24, 1.27, and 1.83, respectively. The rate of heart failure admissions declined after TAVR (incidence rate ratio, 0.55 [95% CI, 0.48-0.62], P<0.001) and SAVR (incidence rate ratio, 0.76 [95% CI, 0.65-0.88], P<0.001).
Conclusions: In ESRD-HD patients with aortic stenosis, mortality was lower in the short-term with TAVR compared with SAVR but comparable in the mid-term. AVR is associated with an improvement in survival and reduction in heart failure hospitalizations compared with conservative management.
Keywords: aortic stenosis; kidney failure, chronic; mortality; population; prognosis; transcatheter aortic valve replacement.
Conflict of interest statement
Figures
References
-
- Nakatsu T, Minakata K, Tanaka S, Minatoya K, Investigators PR- K. Intermediate-term outcomes of aortic valve replacement with bioprosthetic or mechanical valves in patients on hemodialysis. J Thorac Cardiovasc Surg. 2019;157:2177–2186 e2173 - PubMed
-
- Leon MB, Smith CR, Mack MJ, Makkar RR, Svensson LG, Kodali SK, Thourani VH, Tuzcu EM, Miller DC, Herrmann HC, et al. Transcatheter or surgical aortic-valve replacement in intermediate-risk patients. N Engl J Med. 2016;374:1609–1620 - PubMed
-
- Reardon MJ, Van Mieghem NM, Popma JJ, Kleiman NS, Sondergaard L, Mumtaz M, Adams DH, Deeb GM, Maini B, Gada H, et al. Surgical or transcatheter aortic-valve replacement in intermediate-risk patients. N Engl J Med. 2017;376:1321–1331 - PubMed
-
- Alkhalil A, Golbari S, Song D, Lamba H, Fares A, Alaiti A, Deo S, Attizzani GF, Ibrahim H, Ruiz CE. In-hospital outcomes of transcatheter versus surgical aortic valve replacement in end stage renal disease. Catheter Cardiovasc Interv. 2018;92:757–765 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
