

Rates and causes of mortality among children and young people with and without intellectual disabilities in Scotland: a record linkage cohort study of 796 190 school children
- PMID: 32773385
- PMCID: PMC7418667
- DOI: 10.1136/bmjopen-2019-034077
Rates and causes of mortality among children and young people with and without intellectual disabilities in Scotland: a record linkage cohort study of 796 190 school children
Abstract
Objectives: To investigate mortality rates and causes in children and young people with intellectual disabilities.
Design: Retrospective cohort; individual record linkage between Scotland's annual pupil census and National Records of Scotland death register.
Setting: General community.
Participants: Pupils receiving local authority-funded schooling in Scotland, 2008 to 2013, with an Additional Support Need due to intellectual disabilities, compared with other pupils.
Main outcome measures: Deaths up to 2015: age of death, age-standardised mortality ratios (age-SMRs); causes of death including cause-specific age-SMRs; avoidable deaths as defined by the UK Office of National Statistics.
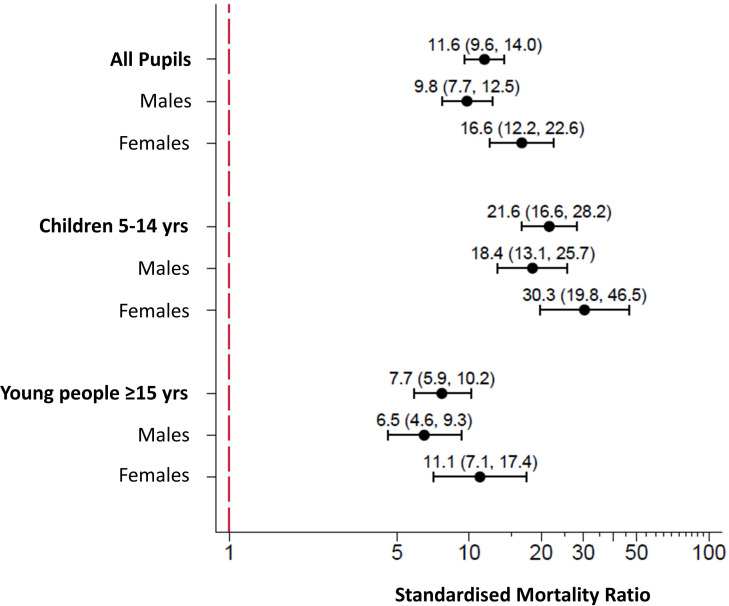
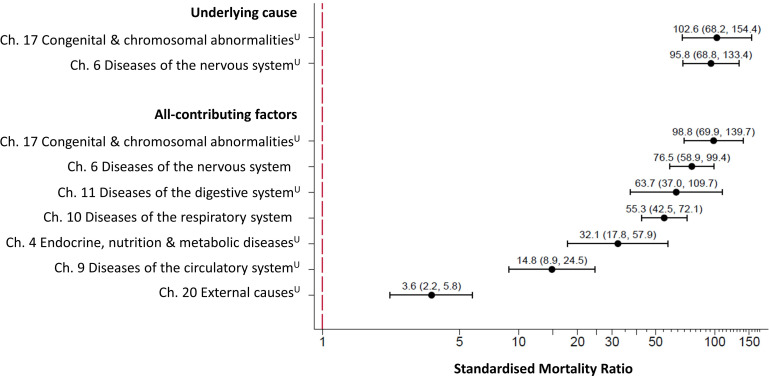
Results: 18 278/947 922 (1.9%) pupils had intellectual disabilities. 106 died over 67 342 person-years (crude mortality rate=157/100 000 person-years), compared with 458 controls over 3 672 224 person-years (crude mortality rate=12/100 000 person-years). Age-SMR was 11.6 (95% CI 9.6 to 14.0); 16.6 (95% CI 12.2 to 22.6) for female pupils and 9.8 (95% CI 7.7 to 12.5) for male pupils. Most common main underlying causes were diseases of the nervous system, followed by congenital anomalies; most common all-contributing causes were diseases of the nervous system, followed by respiratory system; most common specific contributing causes were cerebral palsy, pneumonia, respiratory failure and epilepsy. For all contributing causes, SMR was 98.8 (95% CI 69.9 to 139.7) for congenital anomalies, 76.5 (95% CI 58.9 to 99.4) for nervous system, 63.7 (95% CI 37.0 to 109.7) for digestive system, 55.3 (95% CI 42.5 to 72.1) for respiratory system, 32.1 (95% CI 17.8 to 57.9) for endocrine and 14.8 (95% CI 8.9 to 24.5) for circulatory system. External causes accounted for 46% of control deaths, but the SMR for external-related deaths was still higher (3.6 (95% CI 2.2 to 5.8)) for pupils with intellectual disabilities. Deaths amenable to good care were common.
Conclusion: Pupils with intellectual disabilities were much more likely to die than their peers, and had a different pattern of causes, including amenable deaths across a wide range of disease categories. Improvements are needed to reduce amenable deaths, for example, epilepsy-related and dysphagia, and to support families of children with life-limiting conditions.
Keywords: children; death; intellectual disabilities; mortality; young people.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Hughes-McCormack LA, Rydzewska E, Henderson A, et al. Prevalence of mental health conditions and relationship with general health in a whole-country population of people with intellectual disabilities compared with the general population. BJPsych Open 2017. b;3:243–8. 10.1192/bjpo.bp.117.005462 - DOI - PMC - PubMed