

ACG Clinical Guidelines: Diagnosis and Management of Achalasia
- PMID: 32773454
- PMCID: PMC9896940
- DOI: 10.14309/ajg.0000000000000731
ACG Clinical Guidelines: Diagnosis and Management of Achalasia
Abstract
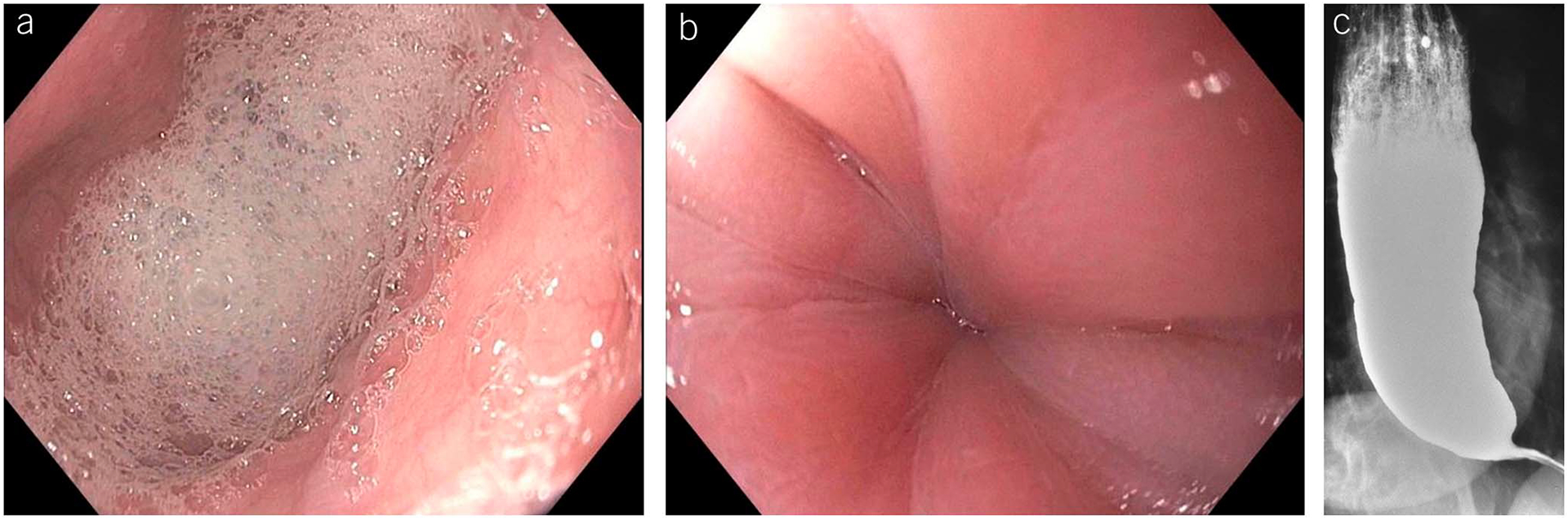
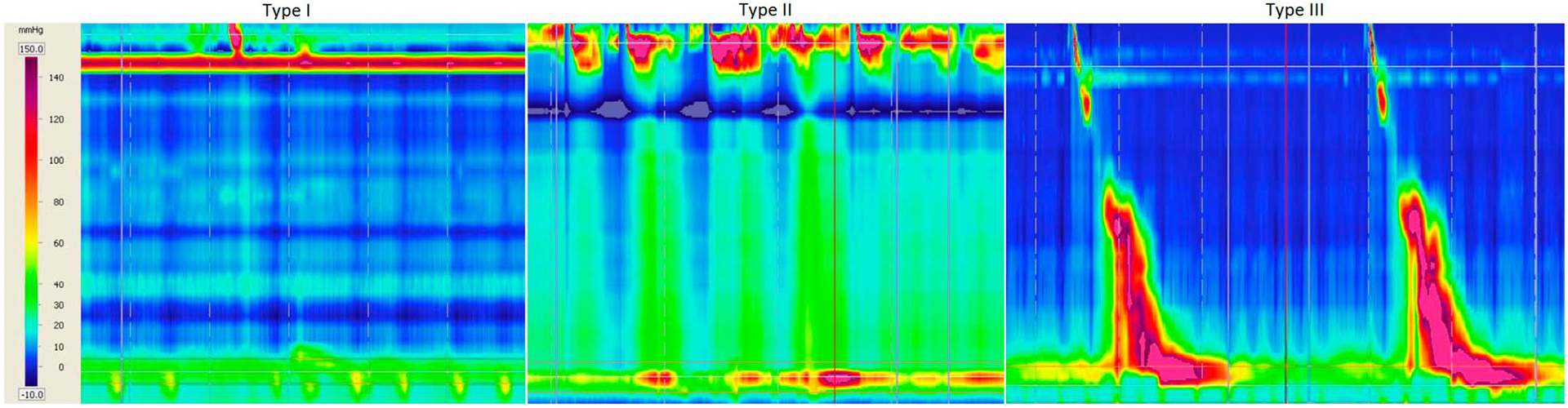
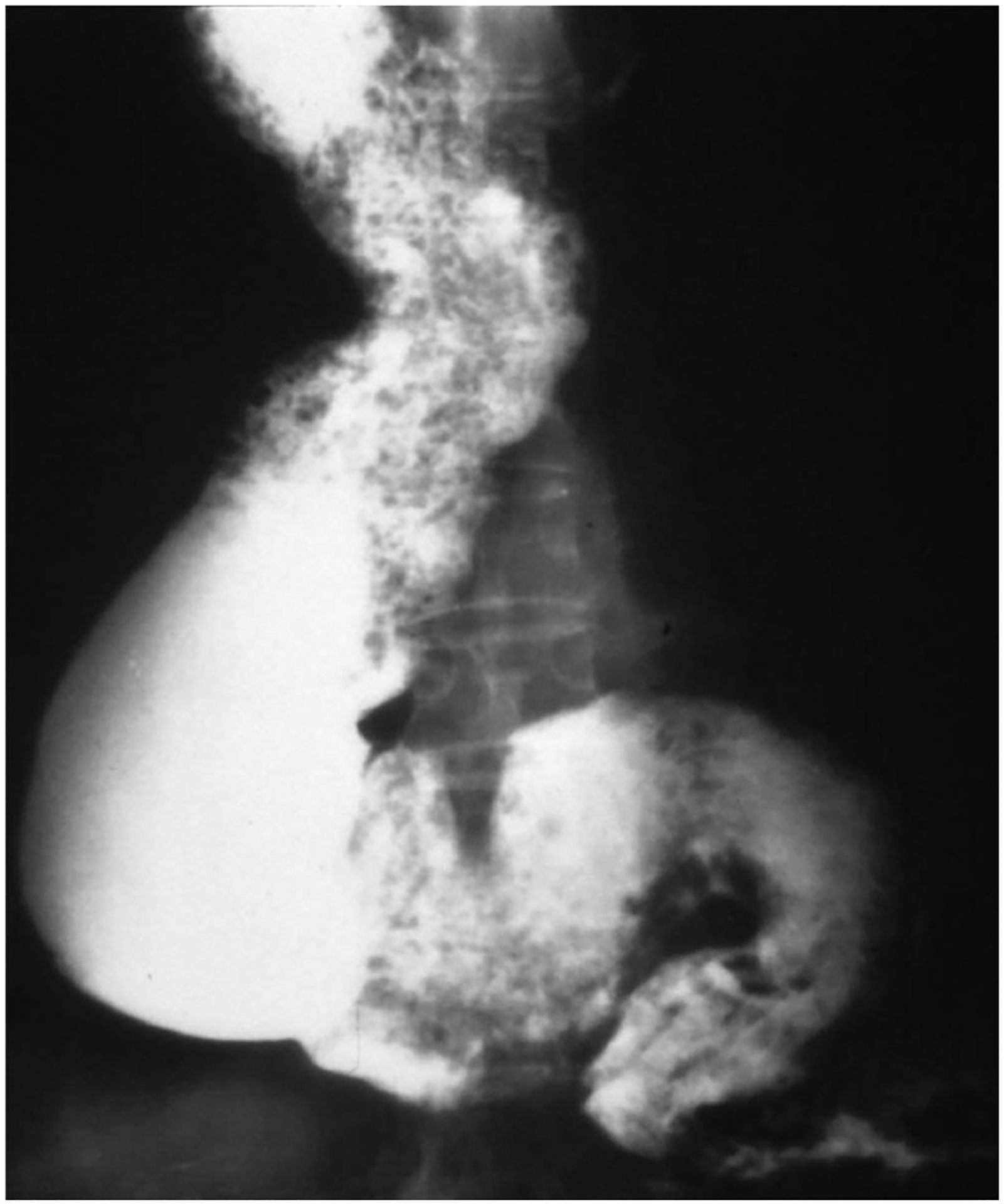
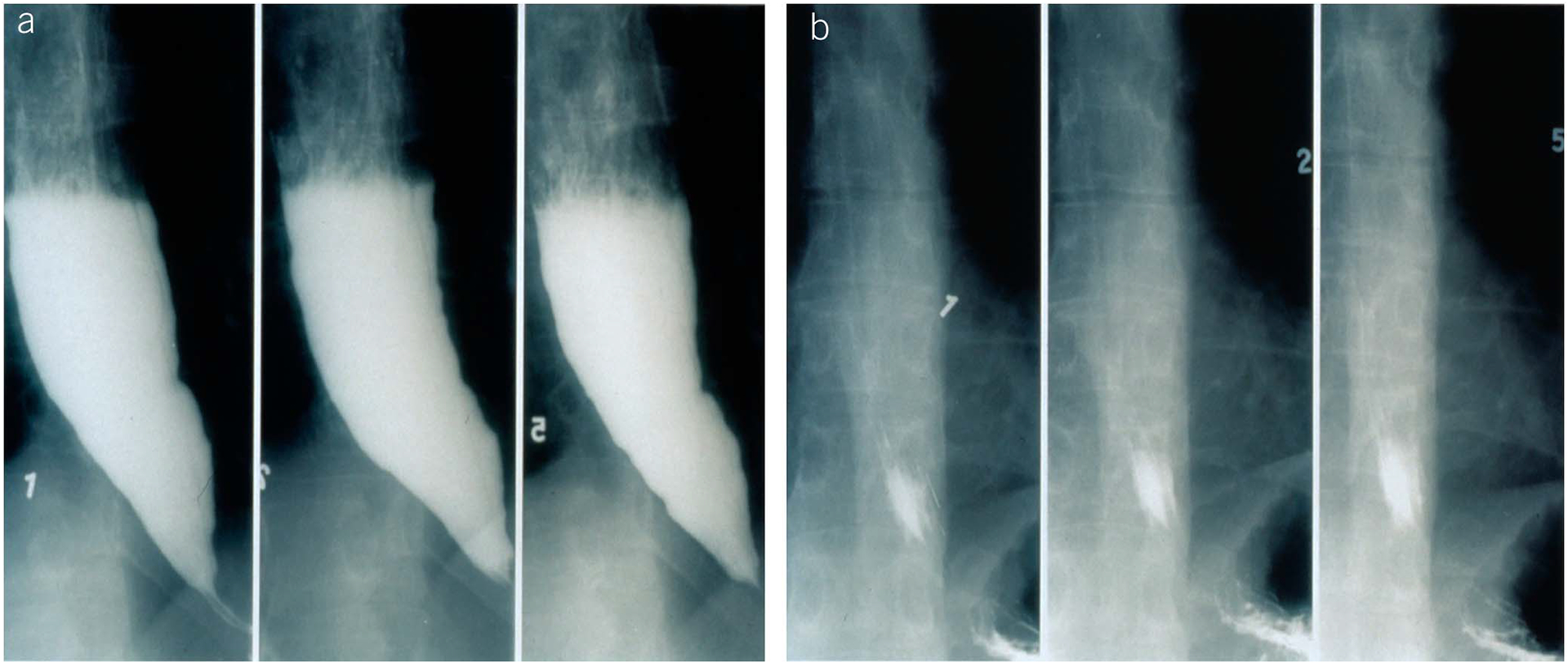
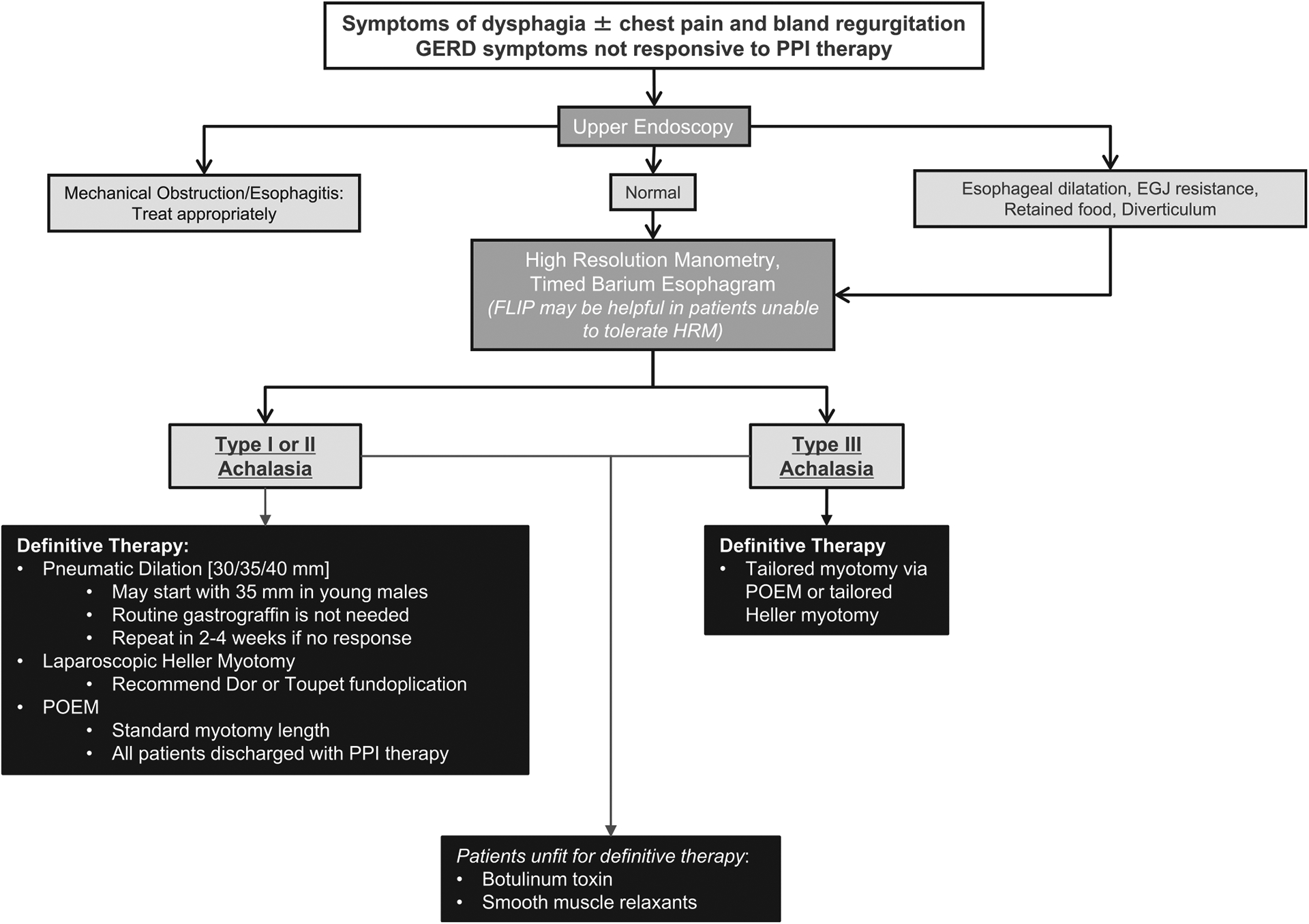
Achalasia is an esophageal motility disorder characterized by aberrant peristalsis and insufficient relaxation of the lower esophageal sphincter. Patients most commonly present with dysphagia to solids and liquids, regurgitation, and occasional chest pain with or without weight loss. High-resolution manometry has identified 3 subtypes of achalasia distinguished by pressurization and contraction patterns. Endoscopic findings of retained saliva with puckering of the gastroesophageal junction or esophagram findings of a dilated esophagus with bird beaking are important diagnostic clues. In this American College of Gastroenterology guideline, we used the Grading of Recommendations Assessment, Development and Evaluation process to provide clinical guidance on how best to diagnose and treat patients with achalasia.
Conflict of interest statement
Figures
References
-
- Vaezi MF, Pandolfino JE, Vela MF. ACG clinical guideline: Diagnosis and management of achalasia. Am J Gastroenterol 2013;108(8):1238–49; quiz 50. - PubMed
-
- Vaezi MF, Felix VN, Penagini R, et al. Achalasia: From diagnosis to management. Ann N Y Acad Sci 2016;1381(1):34–44. - PubMed
-
- Francis DL, Katzka DA. Achalasia: Update on the disease and its treatment. Gastroenterology 2010;139(2):369–74. - PubMed
