

The potential for overdiagnosis and underdiagnosis because of blood pressure variability: a comparison of the 2017 ACC/AHA, 2018 ESC/ESH and 2019 NICE hypertension guidelines
- PMID: 32773652
- PMCID: PMC7810411
- DOI: 10.1097/HJH.0000000000002614
The potential for overdiagnosis and underdiagnosis because of blood pressure variability: a comparison of the 2017 ACC/AHA, 2018 ESC/ESH and 2019 NICE hypertension guidelines
Abstract
Objective: To estimate the extent that BP measurement variability may drive over- and underdiagnosis of 'hypertension' when measurements are made according to current guidelines.
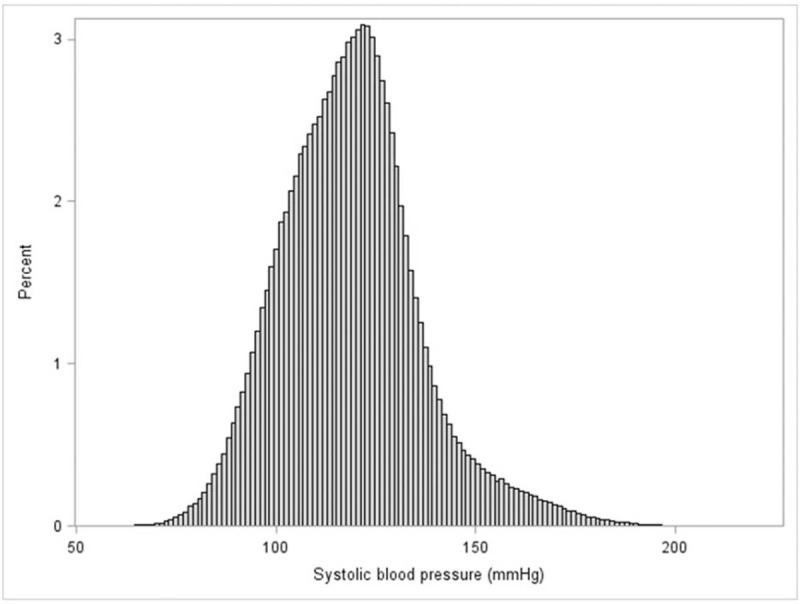
Methods: Using data from the National Health and Nutrition Examination Survey and empirical estimates of within-person variability, we simulated annual SBP measurement sets for 1 000 000 patients over 5 years. For each measurement set, we used an average of multiple readings, as recommended by guidelines.
Results: The mean true SBP for the simulated population was 118.8 mmHg with a standard deviation of 17.5 mmHg. The proportion overdiagnosed with 'hypertension' after five sets of office or nonoffice measurements using the 2017 American College of Cardiology guideline was 3-5% for people with a true SBP less than 120 mmHg, and 65-72% for people with a true SBP 120-130 mmHg. These proportions were less than 1% and 14-33% using the 2018 European Society of Hypertension and 2019 National Institute for Health and Care Excellence guidelines (true SBP <120 and 120-130 mmHg, respectively). The proportion underdiagnosed with 'hypertension' was less than 3% for people with true SBP at least 140 mmHg after one set of office or nonoffice measurements using the 2017 American College of Cardiology guideline, and less than 18% using the other two guidelines.
Conclusion: More people are at risk of overdiagnosis under the 2017 American College of Cardiology guideline than the other two guidelines, even if nonoffice measurements are used. Making clinical decisions about cardiovascular prediction based primarily on absolute risk, minimizes the impact of blood pressure variability on overdiagnosis.
Copyright © 2020 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
There are no conflicts of interest.
Figures
Comment in
-
Understanding the impact of blood pressure guidelines and variability on hypertension diagnoses.J Hypertens. 2021 May 1;39(5):1044-1045. doi: 10.1097/HJH.0000000000002780. J Hypertens. 2021. PMID: 33824260 No abstract available.
-
Reply.J Hypertens. 2021 May 1;39(5):1045-1046. doi: 10.1097/HJH.0000000000002781. J Hypertens. 2021. PMID: 33824261 No abstract available.
References
-
- Brodersen J, Schwartz LM, Heneghan C, O'Sullivan JW, Aronson JK, Woloshin S. Overdiagnosis: what it is and what it isn’t. BMJ Evid Based Med 2018; 23:1–3. - PubMed
-
- Carter SM, Degeling C, Doust J, Barratt A. A definition and ethical evaluation of overdiagnosis. J Med Ethics 2016; 42:705–714. - PubMed
-
- Bell KJL, Doust J, Glasziou P, Cullen L, Harris IA, Smith L, et al. Recognizing the potential for overdiagnosis: are high-sensitivity cardiac troponin assays an example? Recognizing the potential for overdiagnosis. Ann Intern Med 2019; 170:259–261. - PubMed
-
- Doust J, Vandvik PO, Qaseem A, Mustafa RA, Horvath AR, Frances A, et al. Guidelines International Network (G-I-N) Preventing Overdiagnosis Working Group. Guidance for modifying the definition of diseases: a checklist. JAMA Intern Med 2017; 177:1020–1025. - PubMed
-
- Doust JA, Bell KJL, Glasziou PP. Potential consequences of changing disease classifications. JAMA 2020; 323:921–922. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
