

Pulmonary Rehabilitation for Chronic Obstructive Pulmonary Disease: Highly Effective but Often Overlooked
- PMID: 32773722
- PMCID: PMC7515680
- DOI: 10.4046/trd.2020.0064
Pulmonary Rehabilitation for Chronic Obstructive Pulmonary Disease: Highly Effective but Often Overlooked
Abstract
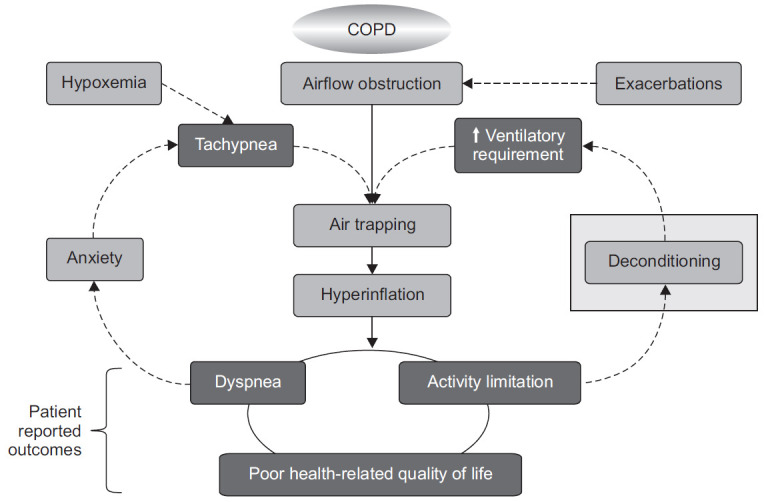
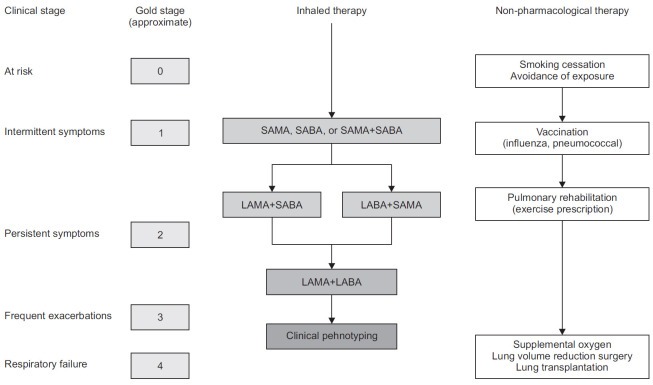
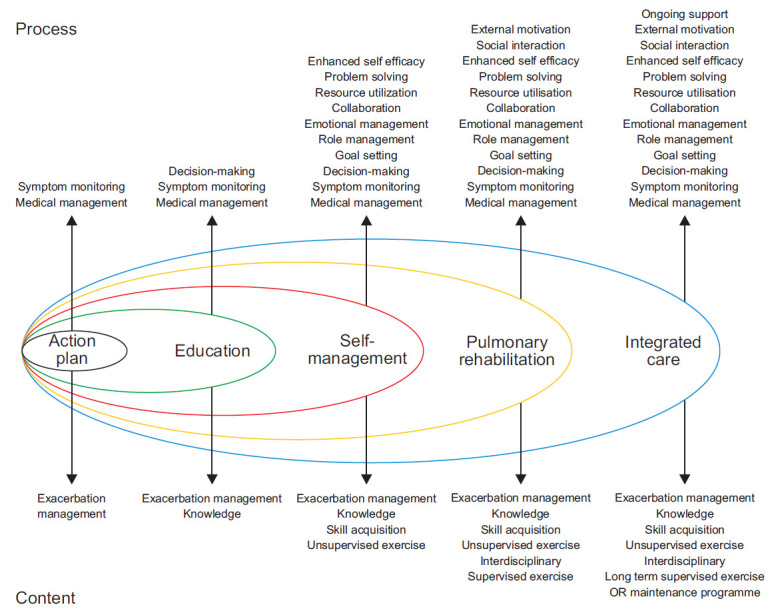
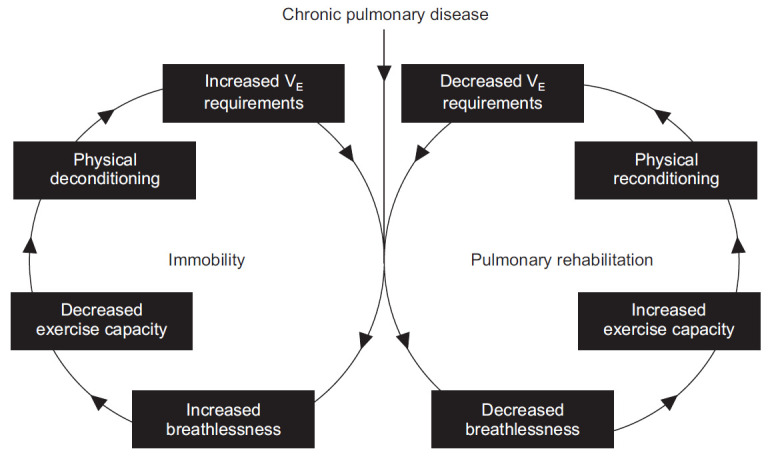
Patients with chronic obstructive pulmonary disease receive a range of treatments including but not limited to inhaled bronchodilators, inhaled and systemic corticosteroids, supplemental oxygen, and pulmonary rehabilitation. Pulmonary rehabilitation is a multidisciplinary intervention that seeks to combine patient education, exercise, and lifestyle changes into a comprehensive program. Programs 6 to 8 weeks in length have been shown to improve health, reduce dyspnea, increase exercise capacity, improve psychological well-being, and reduce healthcare utilization and hospitalization. Although the use of pulmonary rehabilitation is widely supported by the literature, controversy still exists regarding what should be included in the programs. The goal of this review was to summarize the evidence for pulmonary rehabilitation and identify the areas that hold promise in improving its utilization and effectiveness.
Keywords: Exercise Limitation; Exercise Prescription; Pulmonary Rehabilitation; Pulmonary Disease, Chronic Obstructive.
Conflict of interest statement
MTA and BAD report no conflicts of interest. CBC reports grants from NIH/NHLBI, grants from Foundation NIH, grants from COPD Foundation, personal fees from PulmonX, GlaxoSmithKline, NUVAIRA and MGC Diagnostics, outside the submitted work.
Figures
References
-
- World Health Organization . Geneva: World Health Organization; 2020. Disease burden and mortality estimates [Internet] [cited 2020 Jun 14]. Available from: https://www.who.int/healthinfo/global_burden_disease/estimates/en/
-
- Witek TJ, Jr, Mahler DA. Minimal important difference of the transition dyspnoea index in a multinational clinical trial. Eur Respir J. 2003;21:267–72. - PubMed
-
- Waschki B, Kirsten AM, Holz O, Mueller KC, Schaper M, Sack AL, et al. Disease progression and changes in physical activity in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2015;192:295–306. - PubMed
-
- Global Initiative for chronic Obstructive Lung Disease (GOLD) Fontana, WI: GOLD; 2020. Global strategy for the diagnosis, management, and prevention of COPD [Internet] [cited 2020 Jun 14]. Available from: https://goldcopd.org/wp-content/uploads/2019/12/GOLD-2020-FINAL-ver1.2-0....
-
- Pitta F, Troosters T, Spruit MA, Probst VS, Decramer M, Gosselink R. Characteristics of physical activities in daily life in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2005;171:972–7. - PubMed
