

Lymphatic Anatomy and Physiology
- PMID: 32773948
- PMCID: PMC7394563
- DOI: 10.1055/s-0040-1713440
Lymphatic Anatomy and Physiology
Abstract
Lymphatics have long been overshadowed by the remainder of the circulatory system. Historically, lymphatics were difficult to study because of their small and indistinct vessels, colorless fluid contents, and limited effective interventions. However, the past several decades have brought increased funding, advanced imaging technologies, and novel interventional techniques to the field. Understanding the history of lymphatic anatomy and physiology is vital to further realize the role lymphatics play in most major disease pathologies and innovate interventional solutions for them.
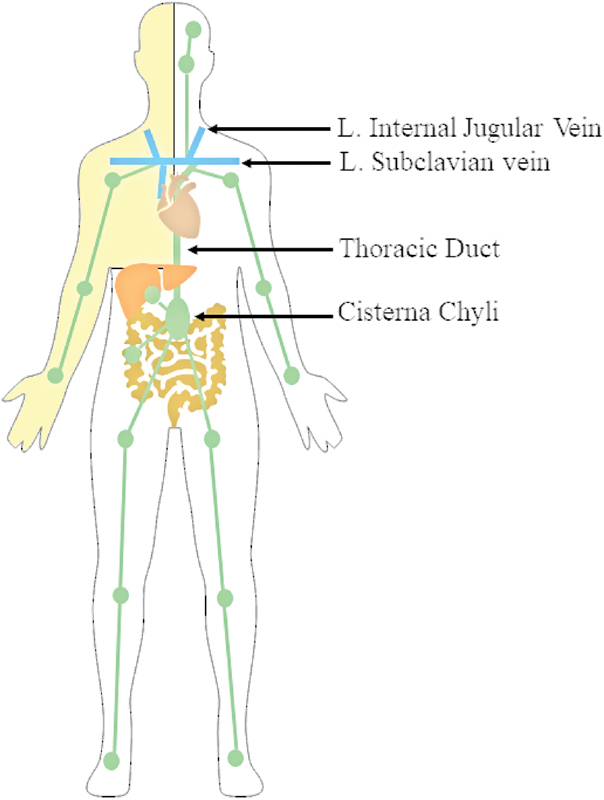
Keywords: anatomy; cisterna chyli; interventional radiology; lymph node; lymphatic; thoracic duct.
© Thieme Medical Publishers.
Conflict of interest statement
Conflict of Interest None declared.
Figures





References
-
- Renkin E M.Some consequences of capillary permeability to macromolecules: Starlings hypothesis reconsideredAm J Physiol Heart Circ Physiol1986. 250(05): - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
