

ROS-Mediated Therapeutic Strategy in Chemo-/Radiotherapy of Head and Neck Cancer
- PMID: 32774675
- PMCID: PMC7396055
- DOI: 10.1155/2020/5047987
ROS-Mediated Therapeutic Strategy in Chemo-/Radiotherapy of Head and Neck Cancer
Abstract
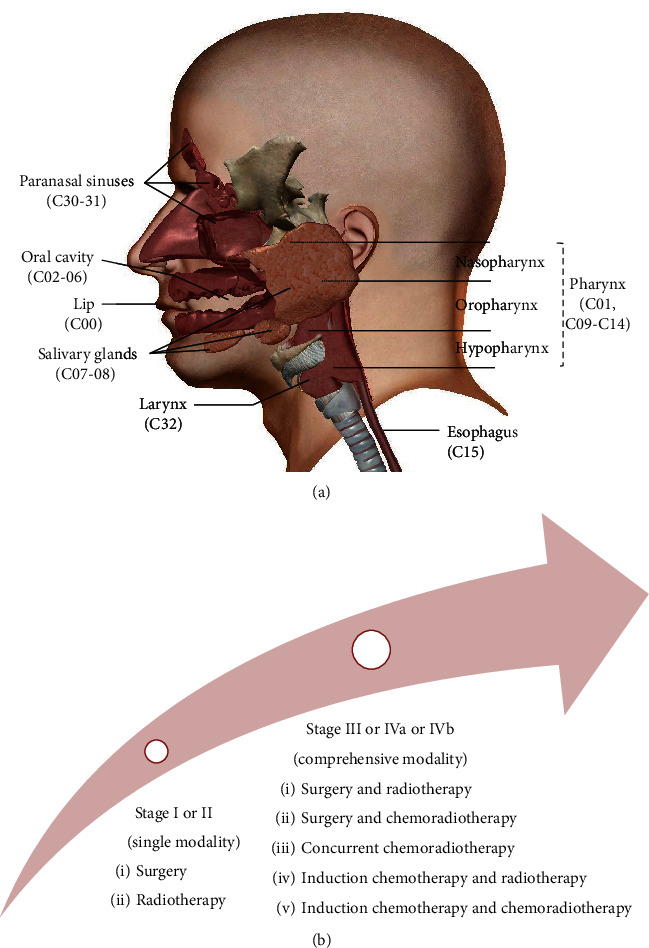
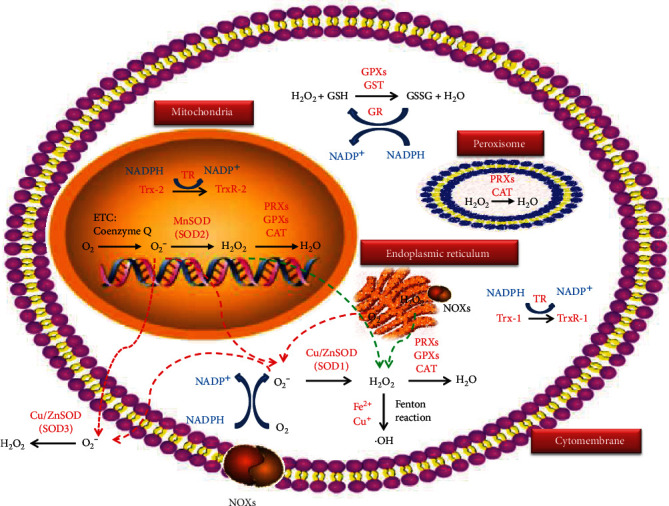
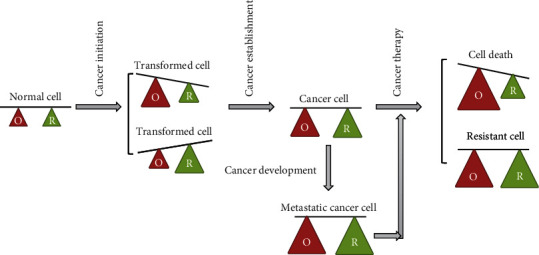
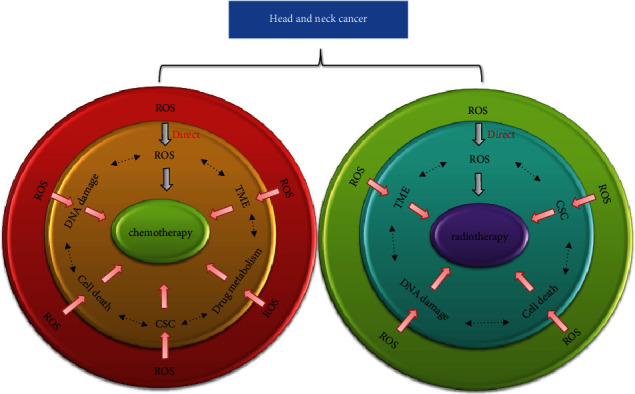
Head and neck cancer is a highly genetic and metabolic heterogeneous collection of malignancies of the lip, oral cavity, salivary glands, pharynx, esophagus, paranasal sinuses, and larynx with five-year survival rates ranging from 12% to 93%. Patients with head and neck cancer typically present with advanced stage III, IVa, or IVb disease and are treated with comprehensive modality including chemotherapy, radiotherapy, and surgery. Despite advancements in treatment modality and technique, noisome recurrence, invasiveness, and resistance as well as posttreatment complications severely influence survival rate and quality of life. Thus, new therapeutic strategies are urgently needed that offer enhanced efficacy with less toxicity. ROS in cancer cells plays a vital role in regulating cell death, DNA repair, stemness maintenance, metabolic reprogramming, and tumor microenvironment, all of which have been implicated in resistance to chemo-/radiotherapy of head and neck cancer. Adjusting ROS generation and elimination to reverse the resistance of cancer cells without impairing normal cells show great hope in improving the therapeutic efficacy of chemo-/radiotherapy of head and neck cancer. In the current review, we discuss the pivotal and targetable redox-regulating system including superoxide dismutases (SODs), tripeptide glutathione (GSH), thioredoxin (Trxs), peroxiredoxins (PRXs), nuclear factor erythroid 2-related factor 2/Kelch-like ECH-associated protein 1 (Nrf2/keap1), and mitochondria electron transporter chain (ETC) complexes and their roles in regulating ROS levels and their clinical significance implicated in chemo-/radiotherapy of head and neck cancer. We also summarize several old drugs (referred to as the non-anti-cancer drugs used in other diseases for a long time) and small molecular compounds as well as natural herbs which effectively modulate cellular ROS of head and neck cancer to synergize the efficacy of conventional chemo-/radiotherapy. Emerging interdisciplinary techniques including photodynamic, nanoparticle system, and Bio-Electro-Magnetic-Energy-Regulation (BEMER) therapy are promising measures to broaden the potency of ROS modulation for the benefit of chemo-/radiotherapy in head and neck cancer.
Copyright © 2020 Gan Huang and Shu-Ting Pan.
Conflict of interest statement
The authors declare that there is no conflict of interest regarding the publication of this paper.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
