

Cardiovascular magnetic resonance in myocardial infarction with non-obstructive coronary arteries patients: A review
- PMID: 32774777
- PMCID: PMC7383353
- DOI: 10.4330/wjc.v12.i6.248
Cardiovascular magnetic resonance in myocardial infarction with non-obstructive coronary arteries patients: A review
Abstract
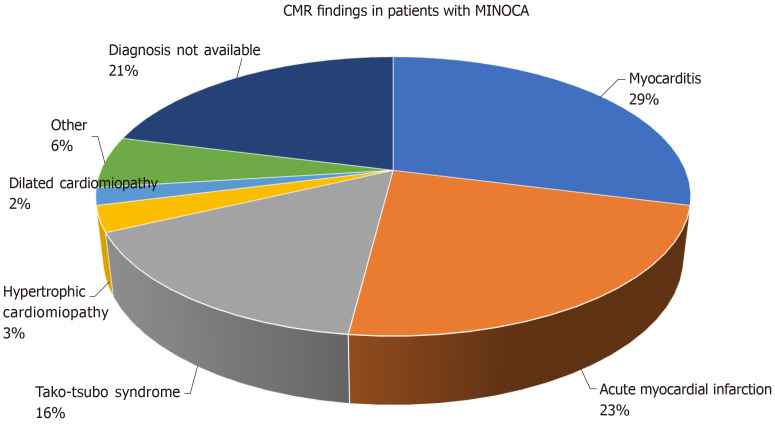
The diagnosis of myocardial infarction with non-obstructive coronary arteries (MINOCA) necessitates documentation of an acute myocardial infarction (AMI), non-obstructive coronary arteries, using invasive coronary angiography or coronary computed tomography angiography and no clinically overt cause for AMI. Historically patients with MINOCA represent a clinical dilemma with subsequent uncertain clinical management. Differential diagnosis is crucial to choose the best therapeutic option for ischemic and non-ischemic MINOCA patients. Cardiovascular magnetic resonance (CMR) is able to analyze cardiac structure and function simultaneously and provides tissue characterization. Moreover, CMR could identify the cause of MINOCA in nearly two-third of patients providing valuable information for clinical decision making. Finally, it allows stratification of patients with worse outcomes which resulted in therapeutic changes in almost half of the patients. In this review we discuss the features of CMR in MINOCA; from exam protocols to imaging findings.
Keywords: Acute coronary syndrome unobstructed coronaries; Acute myocardial infarction; Acute myocarditis; Cardiovascular magnetic resonance; Takotsubo cardiomyopathy.
©The Author(s) 2020. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: The authors have no conflicts of interest to declare.
Figures

Similar articles
-
Prognostic Value of Cardiac Magnetic Resonance Imaging in Patients With a Working Diagnosis of MINOCA-An Outcome Study With up to 10 Years of Follow-Up.Circ Cardiovasc Imaging. 2023 Aug;16(8):e014454. doi: 10.1161/CIRCIMAGING.122.014454. Epub 2023 Aug 15. Circ Cardiovasc Imaging. 2023. PMID: 37582156
-
How to Use Cardiac Magnetic Resonance Imaging in Myocardial Infarction With Nonobstructive Coronary Arteries.Circ Cardiovasc Imaging. 2024 Jul;17(7):e016463. doi: 10.1161/CIRCIMAGING.123.016463. Epub 2024 Jul 16. Circ Cardiovasc Imaging. 2024. PMID: 39012944 Review.
-
Medium-Term Prognostic Implications of Cardiac Magnetic Resonance Imaging in Patients With Myocardial Infarction With Nonobstructive Coronary Arteries (MINOCA): A Systematic Review and Meta-Analysis.Heart Lung Circ. 2023 Nov;32(11):1334-1346. doi: 10.1016/j.hlc.2023.09.007. Epub 2023 Oct 31. Heart Lung Circ. 2023. PMID: 37919116
-
The value of a new cardiac magnetic resonance imaging protocol in Myocardial Infarction with Non-obstructive Coronary Arteries (MINOCA) - a case-control study using historical controls from a previous study with similar inclusion criteria.BMC Cardiovasc Disord. 2017 Jul 24;17(1):199. doi: 10.1186/s12872-017-0611-5. BMC Cardiovasc Disord. 2017. PMID: 28738781 Free PMC article.
-
The Role of Cardiac Magnetic Resonance in Myocardial Infarction and Non-obstructive Coronary Arteries.Front Cardiovasc Med. 2022 Jan 17;8:821067. doi: 10.3389/fcvm.2021.821067. eCollection 2021. Front Cardiovasc Med. 2022. PMID: 35111833 Free PMC article. Review.
Cited by
-
Multi-Modality Deep Infarct: Non-invasive identification of infarcted myocardium using composite in-silico-human data learning.bioRxiv [Preprint]. 2024 Jun 3:2024.05.31.596513. doi: 10.1101/2024.05.31.596513. bioRxiv. 2024. PMID: 38895325 Free PMC article. Preprint.
-
Competency based curriculum for cardiovascular magnetic resonance: A position statement of the Society for Cardiovascular Magnetic Resonance.J Cardiovasc Magn Reson. 2024 Summer;26(1):100006. doi: 10.1016/j.jocmr.2023.100006. Epub 2023 Dec 22. J Cardiovasc Magn Reson. 2024. PMID: 38215698 Free PMC article. Review.
-
Value of a short non-contrast CMR protocol in MINOCA.Eur Radiol. 2024 Feb;34(2):994-1002. doi: 10.1007/s00330-023-10096-2. Epub 2023 Aug 15. Eur Radiol. 2024. PMID: 37581660 Free PMC article.
-
Diffuse Large B-Cell Lymphoma With Cardiac Invasion Presented as Acute Myocardial Infarction and Left Ventricular Hypertrophy: A Case Report.J Investig Med High Impact Case Rep. 2024 Jan-Dec;12:23247096241253334. doi: 10.1177/23247096241253334. J Investig Med High Impact Case Rep. 2024. PMID: 38747509 Free PMC article.
-
Clinical presentation and management of myocardial infarction with nonobstructive coronary arteries (MINOCA): A literature review.Heliyon. 2021 Nov 11;7(11):e08362. doi: 10.1016/j.heliyon.2021.e08362. eCollection 2021 Nov. Heliyon. 2021. PMID: 34816048 Free PMC article. Review.
References
-
- Agewall S, Beltrame JF, Reynolds HR, Niessner A, Rosano G, Caforio AL, De Caterina R, Zimarino M, Roffi M, Kjeldsen K, Atar D, Kaski JC, Sechtem U, Tornvall P WG on Cardiovascular Pharmacotherapy. ESC working group position paper on myocardial infarction with non-obstructive coronary arteries. Eur Heart J. 2017;38:143–153. - PubMed
-
- Tornvall P, Gerbaud E, Behaghel A, Chopard R, Collste O, Laraudogoitia E, Leurent G, Meneveau N, Montaudon M, Perez-David E, Sörensson P, Agewall S. Myocarditis or "true" infarction by cardiac magnetic resonance in patients with a clinical diagnosis of myocardial infarction without obstructive coronary disease: A meta-analysis of individual patient data. Atherosclerosis. 2015;241:87–91. - PubMed
-
- Dastidar AG, Baritussio A, De Garate E, Drobni Z, Biglino G, Singhal P, Milano EG, Angelini GD, Dorman S, Strange J, Johnson T, Bucciarelli-Ducci C. Prognostic Role of CMR and Conventional Risk Factors in Myocardial Infarction With Nonobstructed Coronary Arteries. JACC Cardiovasc Imaging. 2019;12:1973–1982. - PubMed
-
- Bière L, Piriou N, Ernande L, Rouzet F, Lairez O. Imaging of myocarditis and inflammatory cardiomyopathies. Arch Cardiovasc Dis. 2019;112:630–641. - PubMed
-
- Lindahl B, Baron T, Erlinge D, Hadziosmanovic N, Nordenskjöld A, Gard A, Jernberg T. Medical Therapy for Secondary Prevention and Long-Term Outcome in Patients With Myocardial Infarction With Nonobstructive Coronary Artery Disease. Circulation. 2017;135:1481–1489. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
