

Efficacy of Diltiazem for the Control of Blood Pressure in Puerperal Patients with Severe Preeclampsia: A Randomized, Single-Blind, Controlled Trial
- PMID: 32774912
- PMCID: PMC7397380
- DOI: 10.1155/2020/5347918
Efficacy of Diltiazem for the Control of Blood Pressure in Puerperal Patients with Severe Preeclampsia: A Randomized, Single-Blind, Controlled Trial
Abstract
Background: Postpartum preeclampsia is a serious disease related to high blood pressure that occurs commonly within the first six days after delivery.
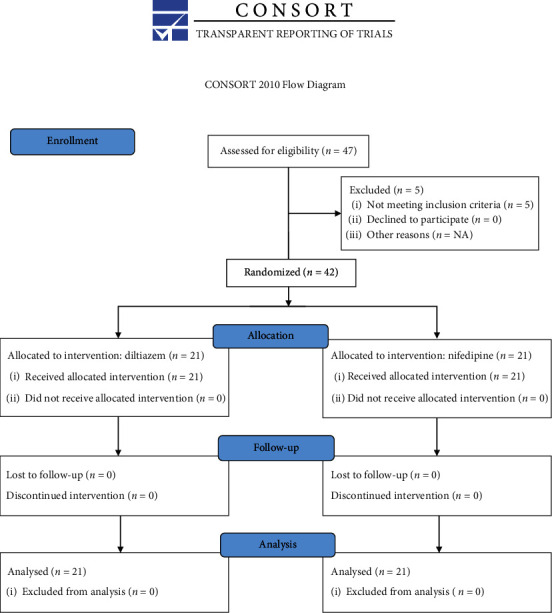
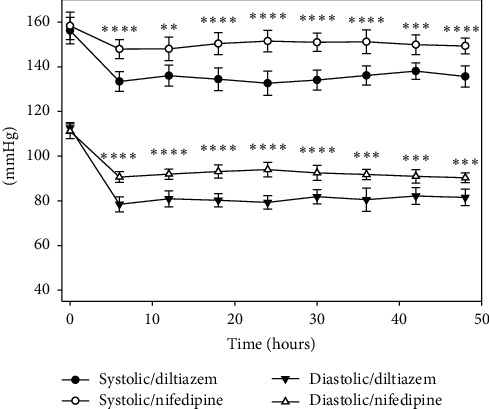
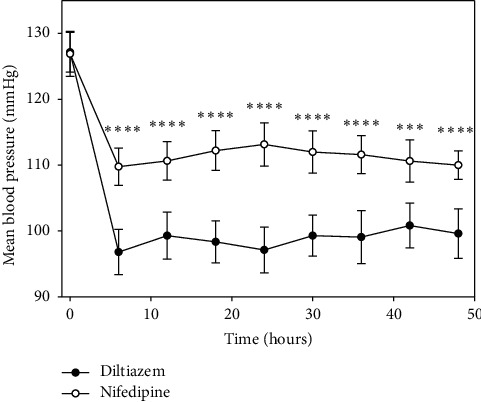
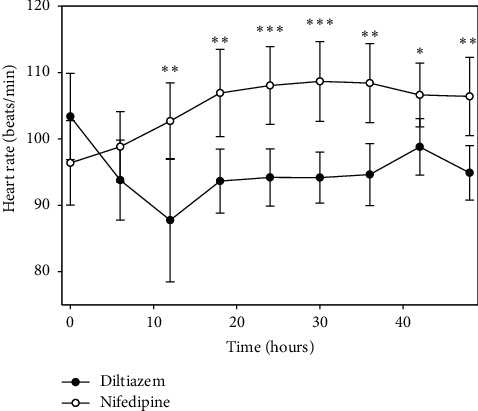
Objective: To evaluate if diltiazem improves blood pressure parameters in early puerperium patients with severe preeclampsia. Methodology. A randomized, single-blind longitudinal clinical trial of 42 puerperal patients with severe preeclampsia was carried out. Patients were randomized into two groups: the experimental group (n = 21) received diltiazem (60 mg) and the control group (n = 21) received nifedipine (10 mg). Both drugs were orally administered every 8 hours. Systolic, diastolic, and mean blood pressures as well as the heart rate were recorded and analyzed (two-way repeated measures ANOVA) at baseline and after 6, 12, 18, 24, 30, 36, 42, and 48 hours. Primary outcome measures were all the aforementioned blood pressure parameters. Secondary outcome measures included the number of hypertension and hypotension episodes along with the length of stay in the intensive care unit.
Results: No statistical differences were found between groups (diltiazem vs. nifedipine) regarding basal blood pressure parameters. Interarm differences in blood pressure (systolic, diastolic, and mean) and heart rate were statistically significant between treatment groups from 6 to 48 hours. Patients in the diltiazem group had lower blood pressure levels than patients in the nifedipine group. Significantly, patients who received diltiazem had fewer hypertension and hypotension episodes and stayed fewer days in the intensive care unit than those treated with nifedipine.
Conclusions: Diltiazem controlled arterial hypertension in a more effective and uniform manner in patients under study than nifedipine. Patients treated with diltiazem had fewer collateral effects and spent less time in the hospital. This trial is registered with NCT04222855.
Copyright © 2020 Gilberto Arias-Hernández et al.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
Associated data
LinkOut - more resources
Full Text Sources
Medical
