

Biomarkers for the Discrimination of Acute Kawasaki Disease From Infections in Childhood
- PMID: 32775314
- PMCID: PMC7388698
- DOI: 10.3389/fped.2020.00355
Biomarkers for the Discrimination of Acute Kawasaki Disease From Infections in Childhood
Abstract
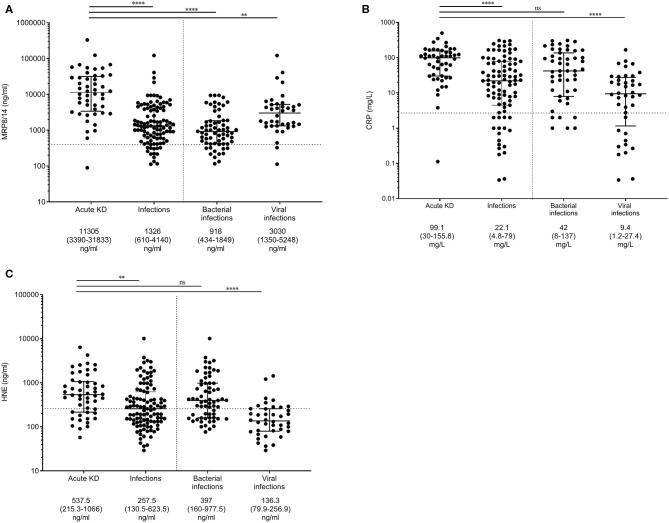
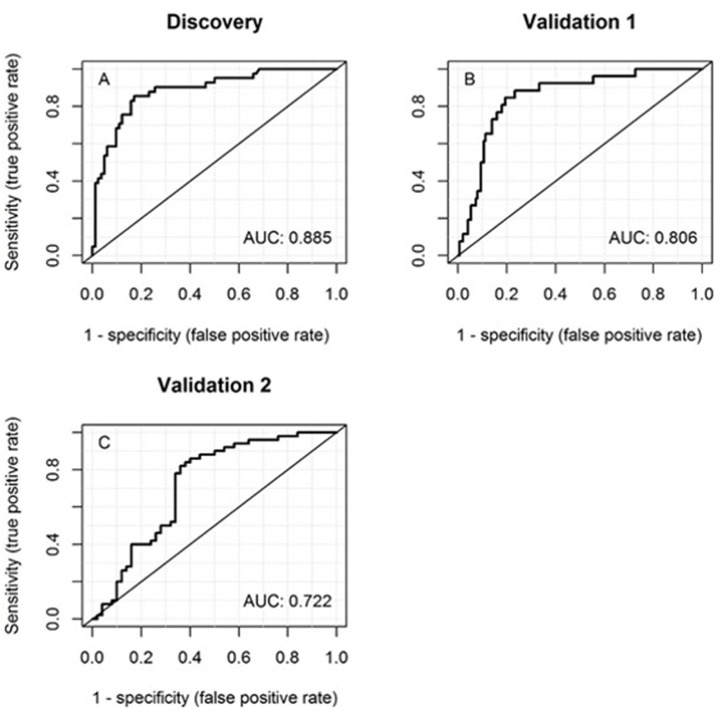
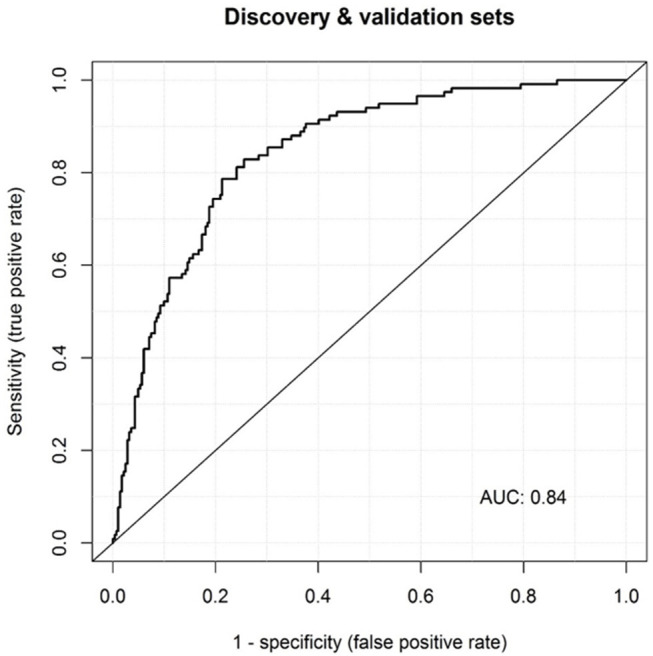
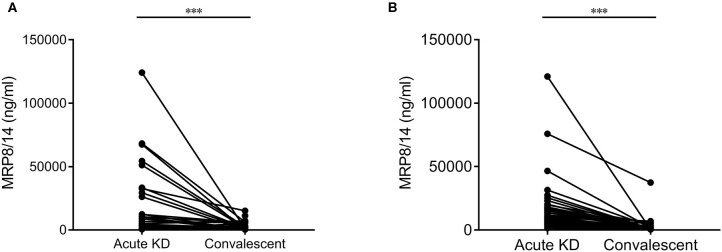
Background: Kawasaki disease (KD) is a vasculitis of early childhood mimicking several infectious diseases. Differentiation between KD and infectious diseases is essential as KD's most important complication-the development of coronary artery aneurysms (CAA)-can be largely avoided by timely treatment with intravenous immunoglobulins (IVIG). Currently, KD diagnosis is only based on clinical criteria. The aim of this study was to evaluate whether routine C-reactive protein (CRP) and additional inflammatory parameters myeloid-related protein 8/14 (MRP8/14 or S100A8/9) and human neutrophil-derived elastase (HNE) could distinguish KD from infectious diseases. Methods and Results: The cross-sectional study included KD patients and children with proven infections as well as febrile controls. Patients were recruited between July 2006 and December 2018 in Europe and USA. MRP8/14, CRP, and HNE were assessed for their discriminatory ability by multiple logistic regression analysis with backward selection and receiver operator characteristic (ROC) curves. In the discovery cohort, the combination of MRP8/14+CRP discriminated KD patients (n = 48) from patients with infection (n = 105), with area under the ROC curve (AUC) of 0.88. The HNE values did not improve discrimination. The first validation cohort confirmed the predictive value of MRP8/14+CRP to discriminate acute KD patients (n = 26) from those with infections (n = 150), with an AUC of 0.78. The second validation cohort of acute KD patients (n = 25) and febrile controls (n = 50) showed an AUC of 0.72, which improved to 0.84 when HNE was included. Conclusion: When used in combination, the plasma markers MRP8/14, CRP, and HNE may assist in the discrimination of KD from both proven and suspected infection.
Keywords: bacterial infection; biomarker; coronary aneurysm; infectious disease; kawasaki disease; vasculitis; viral infection.
Copyright © 2020 Zandstra, van de Geer, Tanck, van Stijn-Bringas Dimitriades, Aarts, Dietz, van Bruggen, Schweintzger, Zenz, Emonts, Zavadska, Pokorn, Usuf, Moll, Schlapbach, Carrol, Paulus, Tsolia, Fink, Yeung, Shimizu, Tremoulet, Galassini, Wright, Martinón-Torres, Herberg, Burns, Levin, Kuijpers, EUCLIDS Consortium, PERFORM Consortium and UK Kawasaki Disease Genetics Study Network.
Figures
Similar articles
-
Interleukin-6 is prone to be a candidate biomarker for predicting incomplete and IVIG nonresponsive Kawasaki disease rather than coronary artery aneurysm.Clin Exp Med. 2019 May;19(2):173-181. doi: 10.1007/s10238-018-00544-5. Epub 2019 Jan 8. Clin Exp Med. 2019. PMID: 30617865
-
The Significance of Symptoms in Predicting Coronary Artery Aneurysms of Kawasaki Disease, Especially in Female Patients.Front Cardiovasc Med. 2022 Apr 28;9:823862. doi: 10.3389/fcvm.2022.823862. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 35571186 Free PMC article.
-
Increased Pentraxin 3 Levels Correlate With IVIG Responsiveness and Coronary Artery Aneurysm Formation in Kawasaki Disease.Front Immunol. 2021 Apr 12;12:624802. doi: 10.3389/fimmu.2021.624802. eCollection 2021. Front Immunol. 2021. PMID: 33912155 Free PMC article.
-
Dissecting Kawasaki disease: a state-of-the-art review.Eur J Pediatr. 2017 Aug;176(8):995-1009. doi: 10.1007/s00431-017-2937-5. Epub 2017 Jun 27. Eur J Pediatr. 2017. PMID: 28656474 Free PMC article. Review.
-
Adjuvant herbal therapy for targeting susceptibility genes to Kawasaki disease: An overview of epidemiology, pathogenesis, diagnosis and pharmacological treatment of Kawasaki disease.Phytomedicine. 2020 Apr 15;70:153208. doi: 10.1016/j.phymed.2020.153208. Epub 2020 Mar 18. Phytomedicine. 2020. PMID: 32283413 Free PMC article. Review.
Cited by
-
Retrospective analysis of children diagnosed with Kawasaki disease.Turk J Med Sci. 2023 Aug;53(4):979-989. doi: 10.55730/1300-0144.5662. Epub 2023 Aug 18. Turk J Med Sci. 2023. PMID: 38031949 Free PMC article.
-
Exploring the diagnostic value of eosinophil-to-lymphocyte ratio to differentiate Kawasaki disease from other febrile diseases based on clinical prediction model.Sci Rep. 2023 Feb 28;13(1):3399. doi: 10.1038/s41598-023-30463-9. Sci Rep. 2023. PMID: 36854770 Free PMC article.
-
Role of Neutrophil Extracellular Traps in Health and Disease Pathophysiology: Recent Insights and Advances.Int J Mol Sci. 2023 Oct 31;24(21):15805. doi: 10.3390/ijms242115805. Int J Mol Sci. 2023. PMID: 37958788 Free PMC article. Review.
-
Lower CMV and EBV Exposure in Children With Kawasaki Disease Suggests an Under-Challenged Immune System.Front Pediatr. 2021 Jan 21;8:627957. doi: 10.3389/fped.2020.627957. eCollection 2020. Front Pediatr. 2021. PMID: 33585370 Free PMC article.
-
Clinical aspects for differential diagnosis of Kawasaki disease shock syndrome: a case control study.BMC Pediatr. 2021 Jan 8;21(1):25. doi: 10.1186/s12887-020-02488-w. BMC Pediatr. 2021. PMID: 33413220 Free PMC article.
References
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous