

Orbital myeloid sarcoma (chloroma): Report of 2 cases and literature review
- PMID: 32775766
- PMCID: PMC7397738
- DOI: 10.1016/j.ajoc.2020.100806
Orbital myeloid sarcoma (chloroma): Report of 2 cases and literature review
Abstract
Purpose: Myeloid sarcoma (MS) of the orbit is an uncommon condition in occurring in children, generally coupled to myeloproliferative neoplasms.
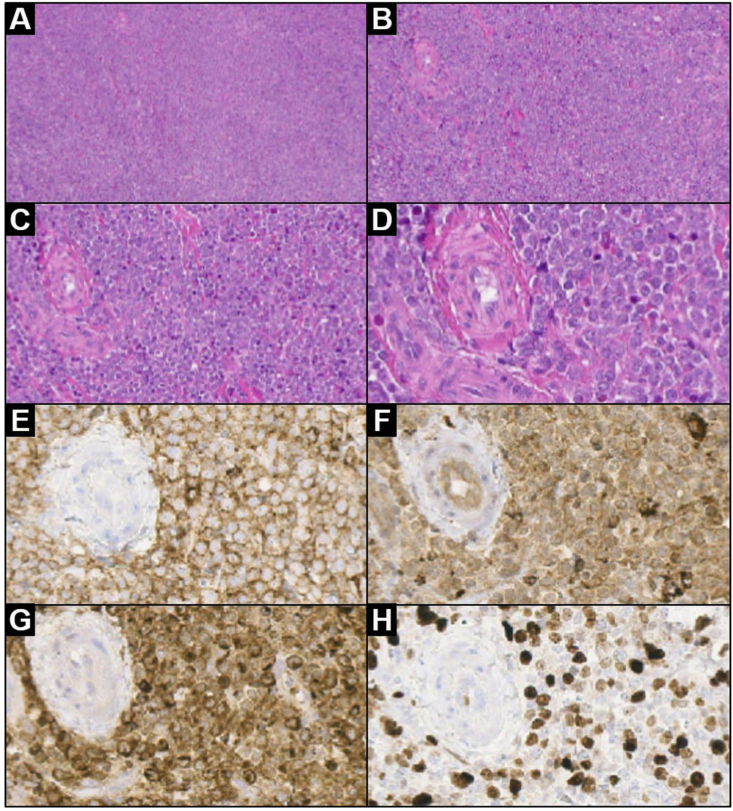
Observations: We describe two rare cases of orbital MS in young boys with aggressive local symptoms but without evidence of acute myeloid leukemia (AML), both patients underwent orbitotomy for gross-tumor resection and biopsy. At follow up, there was no evidence of recurrence nor evolution of the myeloproliferative neoplasms clinically and by radiological and laboratory work-up. We also provide a detailed description of the magnetic resonance imaging presentation, with an extensive pathological analysis correlation.
Conclusions and importance: A comprehensive revision of the literature on isolated orbital MS was carried out with particular emphasis on clues for differential diagnosis and treatment options, stressing the need to consider MS even in the absence of sign and symptoms of an underlying myeloproliferative disorders.
Keywords: Acute myeloid leukemia; Magnetic resonance imaging; Myeloid sarcoma; Orbital pathology; Pediatric tumor.
© 2020 The Authors.
Conflict of interest statement
The following authors have no financial disclosures (MP, MA, CR, HA, AM, SE, RM, MM, AE, LR, RC, DS).
Figures




References
-
- Guermazi A., Feger C., Rousselot P. Granulocytic sarcoma (chloroma): imaging findings in adults and children. AJR. 2002;178(February):319–325. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
