

Urinary Sodium-to-Potassium Ratio and Blood Pressure in CKD
- PMID: 32775823
- PMCID: PMC7403539
- DOI: 10.1016/j.ekir.2020.05.025
Urinary Sodium-to-Potassium Ratio and Blood Pressure in CKD
Abstract
Introduction: In the general population, urinary sodium-to-potassium (uNa/K) ratio associates more strongly with high blood pressure (BP) than either urinary sodium or potassium alone. Whether this is also the case among patients with chronic kidney disease (CKD) is unknown.
Methods: We studied the associations of spot urine sodium-to-creatinine (uNa/Cr), potassium-to-creatinine (uK/Cr), and uNa/K ratios with a single office BP reading in 1660 patients with moderate to severe CKD at inclusion in the CKD-REIN cohort.
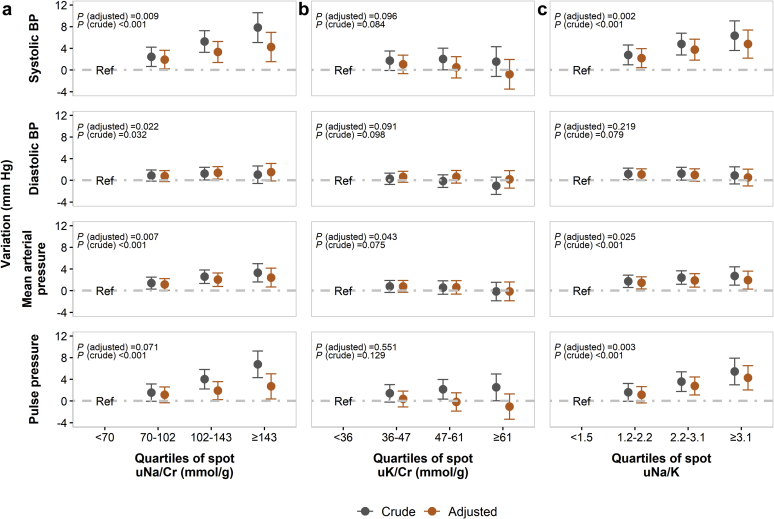
Results: Patients' median age was 68 (interquartile range [IQR], 59-76) years; most were men (65%), had moderate CKD (57%), and albuminuria (72%). Mean systolic and diastolic BP was 142/78 mm Hg. Spot uNa/Cr and uNa/K ratios were positively associated with systolic, mean arterial, and pulse pressures. The mean adjusted difference in systolic BP between the highest and the lowest quartile (Q4 vs. Q1) was 4.24 (95% confidence interval [CI], 1.53-6.96) mm Hg for uNa/Cr and 4.79 (95% CI, 2.18-7.39) mm Hg for uNa/K. Quartiles of spot uK/Cr were not associated with any BP index. The higher the quartile of uNa/K, the higher the prevalence ratio of uncontrolled (Q4 vs. Q1, 1.43; 95% CI, 1.19-1.72) or apparently treatment-resistant hypertension (Q4 vs. Q1, 1.35; 95% CI, 1.14-1.60). Findings were consistent in a subset of 803 individuals with 2 BP readings.
Conclusion: In patients with CKD, higher urinary sodium excretion is associated with higher BP, but unlike in general population, lower potassium excretion is not. Urinary Na/K does not add significant value in assessing high BP risk, except perhaps for hypertension control assessment.
Keywords: blood pressure; chronic kidney disease; potassium; salt; sodium.
© 2020 International Society of Nephrology. Published by Elsevier Inc.
Figures



References
-
- Williams B., Mancia G., Spiering W. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur Heart J. 2018;39:3021–3104. - PubMed
-
- Khaw K.-T., Bingham S., Welch A. Blood pressure and urinary sodium in men and women: the Norfolk Cohort of the European Prospective Investigation into Cancer (EPIC-Norfolk) Am J Clin Nutr. 2004;80:1397–1403. - PubMed
-
- Mente A., O’Donnell M.J., Rangarajan S. Association of urinary sodium and potassium excretion with blood pressure. N Engl J Med. 2014;371:601–611. - PubMed
-
- Welsh C., Welsh P., Jhund P. Urinary sodium excretion, blood pressure, and risk of future cardiovascular disease and mortality in subjects without prior cardiovascular disease. Hypertension. 2019;73:1202–1209. - PubMed
-
- Buendia J.R., Bradlee M.L., Daniels S.R. Longitudinal effects of dietary sodium and potassium on blood pressure in adolescent girls. JAMA Pediatr. 2015;169:560–568. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
