

doi: 10.1016/j.ekir.2020.06.033.
eCollection 2020 Aug.
Dashboards to Facilitate Nephrology Disaster Planning in the COVID-19 Era
Affiliations
- PMID: 32775829
- PMCID: PMC7332958
- DOI: 10.1016/j.ekir.2020.06.033
Item in Clipboard
Dashboards to Facilitate Nephrology Disaster Planning in the COVID-19 Era
Kidney Int Rep.
.
No abstract available
Figures
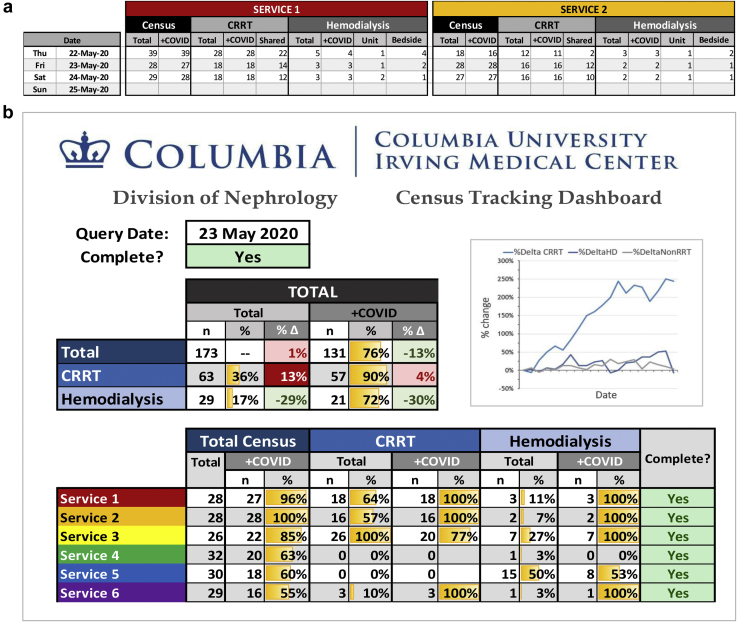
(a) Patient Census Tracker and (b) Dashboard. (a) Each nephrology service (2 of the 6 services shown as an example) reported daily census counts by coronavirus disease (COVID) status and renal replacement therapy (RRT) needs. (b) This populated a division-wide dashboard that summarized the entire divisional service size stratified by COVID status and RRT needs and displays historical growth trends visually by cell color shading and graphically over time. HD, hemodialysis.
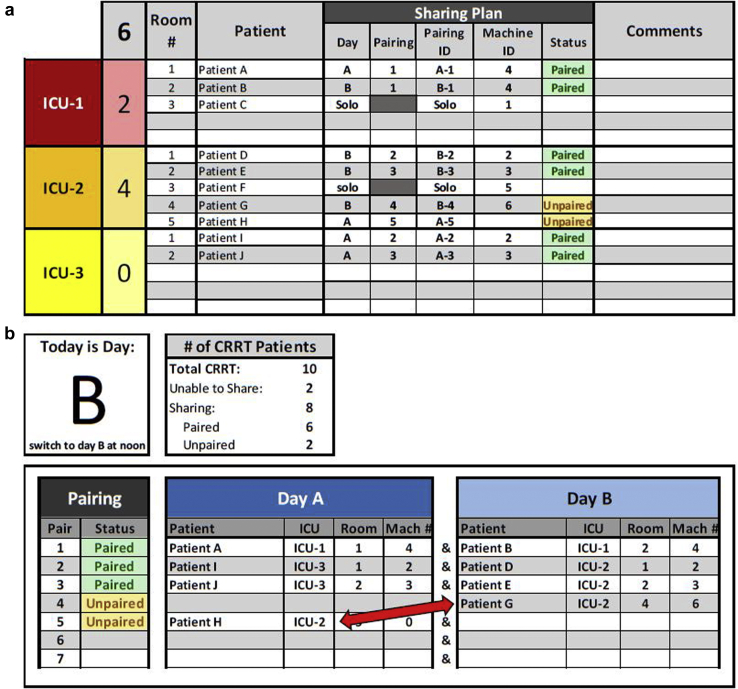
Continuous renal replacement therapy (CRRT) Sharing Protocol Tracker and dashboard. (a) Patients were identified as able to tolerate a sharing protocol (alternating days A and B) or not (solo) by broken down by each intensive care unit (ICU) location. Patients who were unpaired or resources that were overallocated based on their pairing and machine number were visually identified by a color change and allowed clinicians to accurately pair these patients. (b) This information populates the CRRT Sharing Dashboard that detailed names, ICU location, room number, and machine (Mach) number of the 2 patients in a pair, and this information guided coordinators in charge of physically moving the machine from one patient to the next. The dashboard allowed for rapid visual identification of pairing opportunities (e.g. patient G and patient H in ICU-2 can be paired as they are on alternating days [red arrow]).
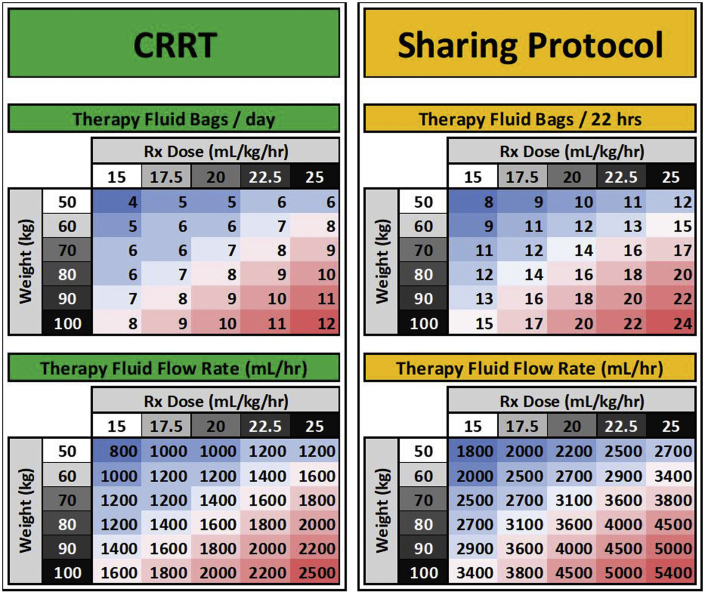
Therapy Fluid Conservation Nomogram. For a given patient weight and prescribed dose, a total therapy fluid volume required session was calculated and rounded up to a 5-L increment (5-L therapy fluid bags). Flow rates for patients on this sharing protocol were determined by adjusting for a 22-hour period. The projected total delivered therapy volume for a standard 48-hour period was adjusted for a 22-hour delivery period (standard flow rates multiplied by 2.18 []) and rounding down to the nearest dl/h. This prevented partially used therapy fluid bags from being discarded at the end of a 22-hour treatment session.
References
-
- Abelson R., Fink S., Kulish N., Thomas K. An overlooked, possibly fatal coronavirus crisis: a dire need for kidney dialysis. New York Times. April 18, 2020 Available at: https://www.nytimes.com/2020/04/18/health/kidney-dialysis-coronavirus.html. Accessed June 2, 2020.
-
- Edrees F., Li T., Vijayan A. Prolonged intermittent renal replacement therapy. Adv Chronic Kidney Dis. 2016;23:195–202. - PubMed
-
- Bellomo R., Baldwin I., Fealy N. Prolonged intermittent renal replacement therapy in the intensive care unit. Crit Care Resusc. 2002;4:281–290. - PubMed
-
- Gashti C.N., Salcedo S., Robinson V., Rodby R.A. Accelerated venovenous hemofiltration: early technical and clinical experience. Am J Kidney Dis. 2008;51:804–810. - PubMed
LinkOut - more resources
Full Text Sources
