

Vitamin D Analogues and Coronary Calcification in CKD Stages 3 and 4: A Randomized Controlled Trial of Calcitriol Versus Paricalcitol
- PMID: 32775985
- PMCID: PMC7406841
- DOI: 10.1016/j.xkme.2020.05.009
Vitamin D Analogues and Coronary Calcification in CKD Stages 3 and 4: A Randomized Controlled Trial of Calcitriol Versus Paricalcitol
Abstract
Rationale & objective: Mineral and bone disorder in chronic kidney disease (CKD) is associated with progression of coronary artery calcification (CAC). Mineral and bone disorder often is treated with calcitriol and other vitamin D receptor activators, including paricalcitol, agents that may have differential effects on calcium, phosphate, and parathyroid hormone levels. Accordingly, we investigated whether these agents have differential effects on CAC progression in patients with CKD.
Study design: Randomized, double-concealed, 48-week clinical trial.
Setting & participants: CKD stage 3 or 4 with secondary hyperparathyroidism with CAC score > 0 and no prior treatment with activated vitamin D.
Intervention: Calcitriol versus paricalcitol.
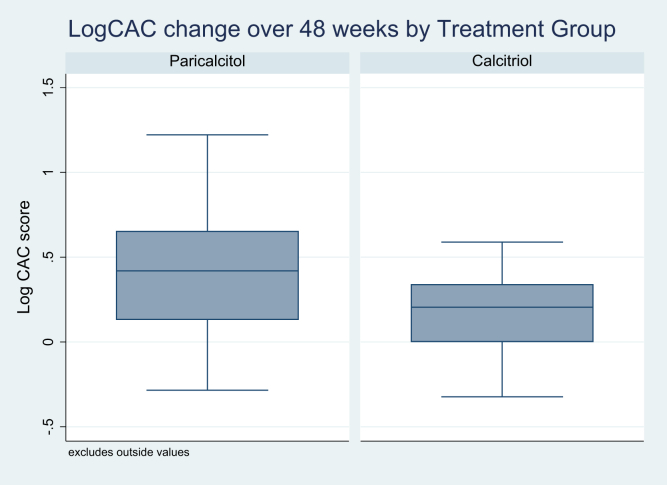
Outcomes: The primary outcome was log-transformed CAC change. Secondary outcomes included percent change in CAC volume, valvular calcifications, and bone mineral metabolism markers.
Results: Among 44 individuals randomly assigned, mean age was 65 years and mean estimated glomerular filtration rate was 27 mL/min/1.73 m2. Median CAC score was 140 (IQR, 55-277) Agatston units at baseline. There was no significant difference in CAC progression between treatment arms (P = 0.06). After adjustment for baseline CAC score (log), treatment group remains nonsignificant (P = 0.08). Further adjustment for creatinine level and/or CKD stage did not change the association. In secondary analyses adjusting for dose level of activated vitamin D, treatment group was significant (P = 0.01), and when dose level was also included in the model, the coefficient for individuals in the paricalcitol group was significantly associated with CAC progression (P = 0.02). An interaction term between dosing level and CKD stage was significant at the highest dosing level (P = 0.04).
Limitations: Pilot single-center study.
Conclusions: In patients with CKD with secondary hyperparathyroidism naive to activated vitamin D therapy, there was no difference in CAC or valvular progression in participants receiving calcitriol compared with paricalcitol during a 48-week period.
Funding: Abbvie, Inc.
Trial registration: NCT00752102.
Keywords: Vascular calcification; activated vitamin D; calcitriol; chronic kidney disease; coronary calcification; paricalcitol.
© 2020 The Authors.
Figures




Comment in
-
Testing Vitamin D Analogues for Vascular Calcification in Patients With CKD.Kidney Med. 2020 Jul 2;2(4):385-387. doi: 10.1016/j.xkme.2020.06.003. eCollection 2020 Jul-Aug. Kidney Med. 2020. PMID: 32779642 Free PMC article. No abstract available.
References
-
- Kasiske B.L. Hyperlipidemia in patients with chronic renal disease. Am J Kidney Dis. 1998;2(5 suppl 3):S142–S156. - PubMed
-
- US Renal Data System . National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases; Bethesda, MD: 2005. USRDS 2005 Annual Data Report.
-
- Kidney Disease: Improving Global Outcomes (KDIGO) CKD-MBD Work Group KDIGO clinical practice guideline for the diagnosis, evaluation, prevention, and treatment of Chronic Kidney Disease-Mineral and Bone Disorder (CKD-MBD) Kidney Int Suppl. 2009;1:S1–S130. - PubMed
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
