

Cases of ROS1-rearranged lung cancer: when to use crizotinib, entrectinib, lorlatinib, and beyond?
- PMID: 32776005
- PMCID: PMC7410006
- DOI: 10.21037/pcm-2020-potb-02
Cases of ROS1-rearranged lung cancer: when to use crizotinib, entrectinib, lorlatinib, and beyond?
Abstract
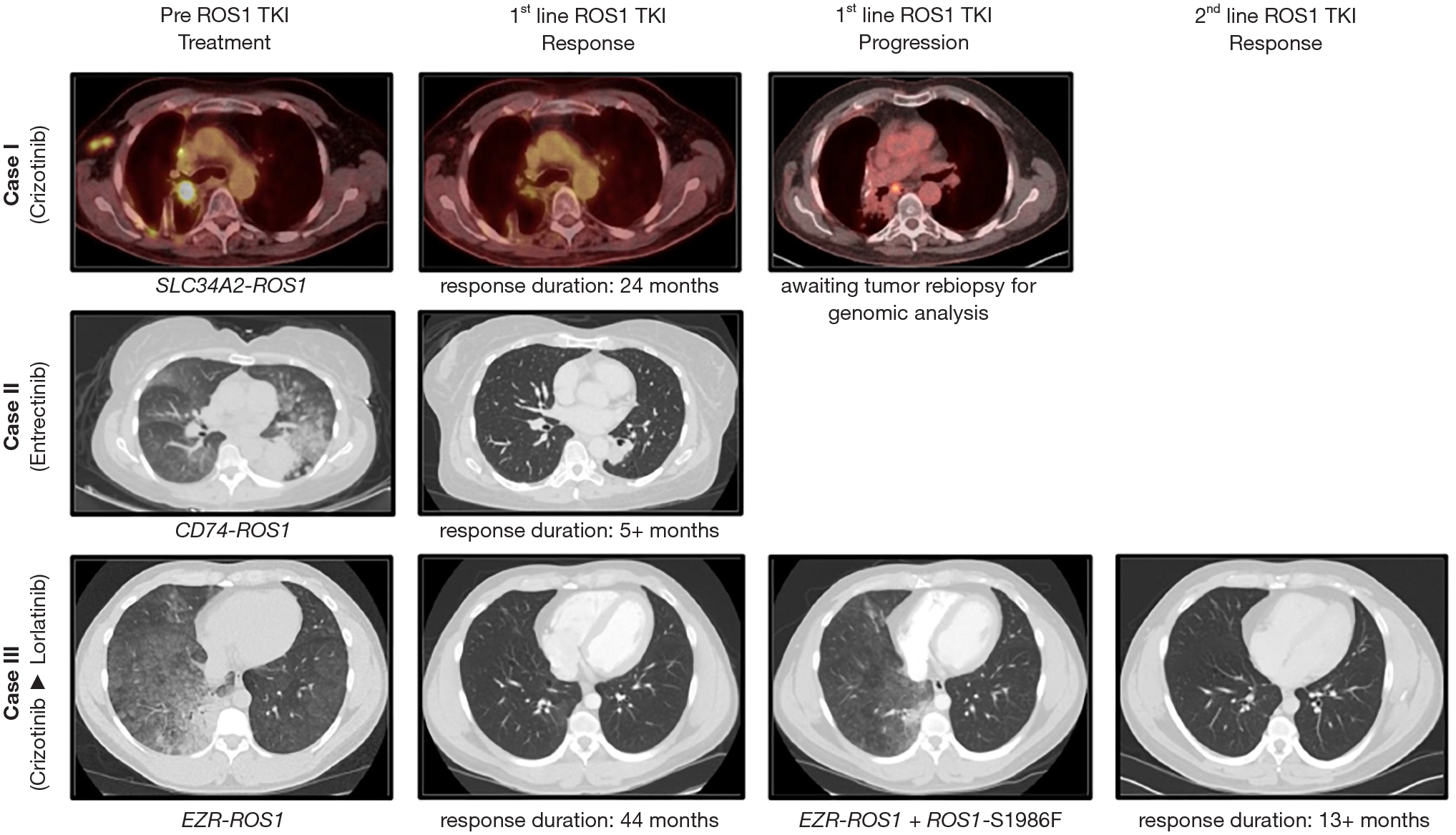
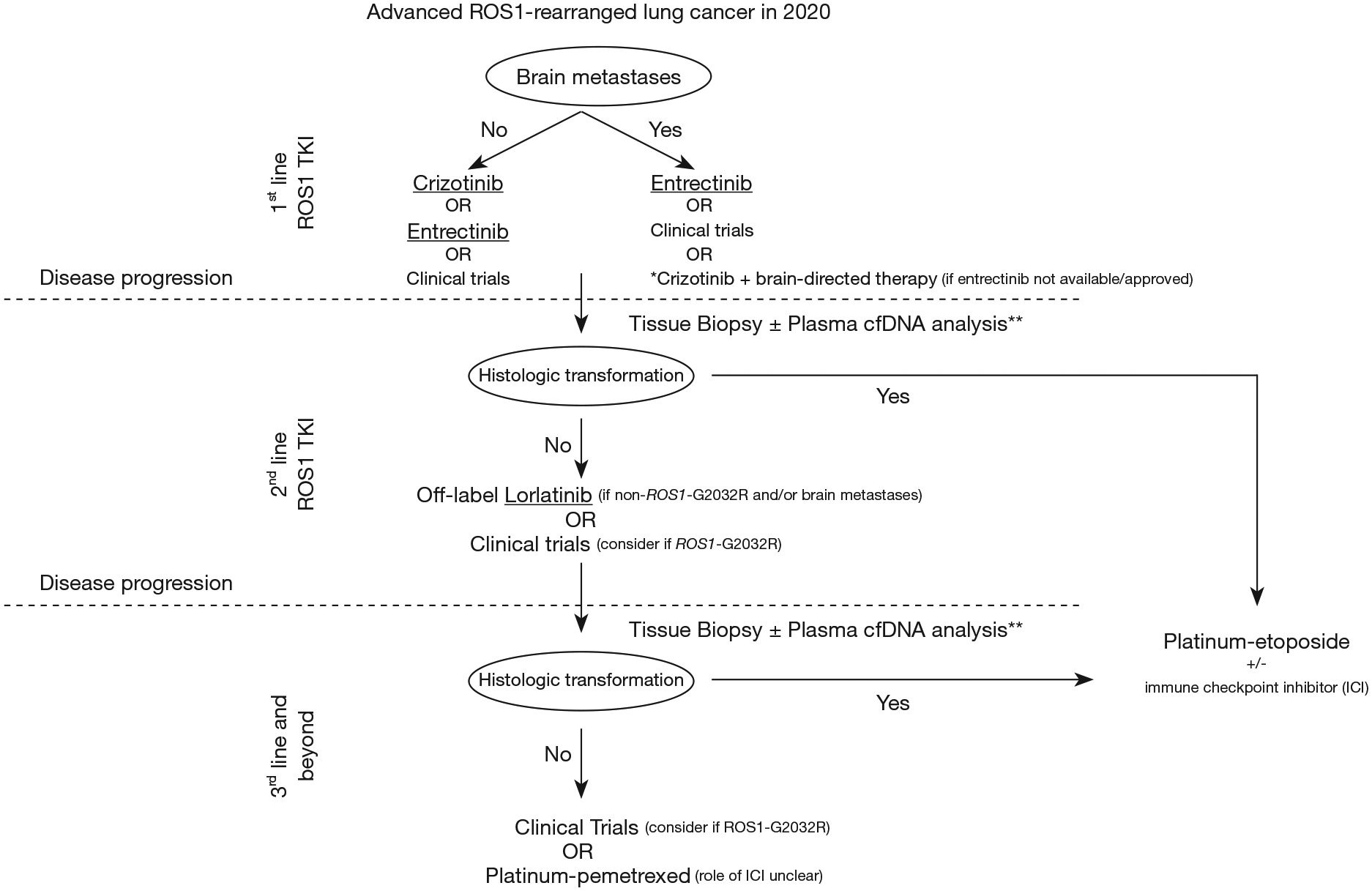
ROS1-rearranged (also known as ROS1 fusion-positive) non-small-cell lung cancer is an uncommon but distinct molecular subgroup seen in approximately 1-2% of cases. Oncogene addiction due to constitutive ROS1 tyrosine kinase activation has allowed development of molecularly targeted therapies with remarkable anti-tumor activity. Both crizotinib and entrectinib, multitargeted tyrosine kinase inhibitors (TKIs) have now received approval by the FDA for treatment of patients with advanced ROS1-rearranged lung cancers; however, the clinical efficacy and safety of these drugs have been derived from expansion cohorts of single-arm phase I or basket clinical trials with relatively small populations of this clinically and molecularly distinct subgroup. Both drugs lead to high objective response rates (approximately 70-80%) and have manageable side effects, although only entrectinib has potent intracranial efficacy. Lorlatinib is an oral brain-penetrant ALK/ROS1 TKI with activity in both TKI-naïve and some crizotinib-resistant settings (albeit with limited potency against the crizotinib/entrectinib-resistant ROS1-G2032R mutation). We describe cases of advanced ROS1-rearranged lung cancer receiving crizotinib, entrectinib, and/or lorlatinib in first and later line treatment settings to dissect the current state of evidence supporting management decisions for these patients. The next generation ROS1 TKIs (repotrectinib and DS-6051b), owing to their broad activity against kinase mutations including ROS1-G2032R in preclinical studies, hold promise to transform the current treatment paradigm and permit even further gains with regards to long-term outcomes in this subset of patients.
Keywords: ROS1 fusion; acquired resistance; crizotinib; entrectinib; lorlatinib; non-small-cell lung cancer (NSCLC); rearrangement.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at http://dx.doi.org/10.21037/pcm-2020-potb-02). The Series “Precision Oncology Tumor Board” was commissioned by the editorial office without any funding or sponsorship. DBC reports personal fees (consulting fees and honoraria) and nonfinancial support (institutional research support) from Takeda/Millennium Pharmaceuticals, and AstraZeneca, and Pfizer, as well as nonfinancial support (institutional research support) from Merck Sharp and Dohme Corporation, Merrimack Pharmaceuticals, Bristol-Myers Squibb, Clovis Oncology, Spectrum Pharmaceuticals and Tesaro, all outside the submitted work. DR reports nonfinancial support (institutional research support) from Bristol-Myers Squibb, Novocure, and Abbvie/Stemcentrx, all outside the submitted work. KS serves as an unpaid editorial board member of Precision Cancer Medicine from Apr 2019 to Mar 2021. The other authors have no conflicts of interest to declare.
Figures
References
-
- Takeuchi K, Soda M, Togashi Y, et al. RET, ROS1 and ALK fusions in lung cancer. Nat Med 2012;18:378–81. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources