

Cardiovascular Effects of CAR T Cell Therapy: A Retrospective Study
- PMID: 32776016
- PMCID: PMC7413146
- DOI: 10.1016/j.jaccao.2020.04.012
Cardiovascular Effects of CAR T Cell Therapy: A Retrospective Study
Abstract
Background: Anti-CD19 chimeric antigen receptor (CAR) T cell (CART19) therapy holds great promise in the treatment of hematological malignancies. A high occurrence of cardiac dysfunction has been noted in children treated with CART19 therapy.
Objectives: We aimed to define the occurrence of major cardiovascular events (MACE) in adult patients treated with CART19 cells and assess the relationships between clinical factors, echocardiographic parameters, laboratory values, and cardiovascular outcomes.
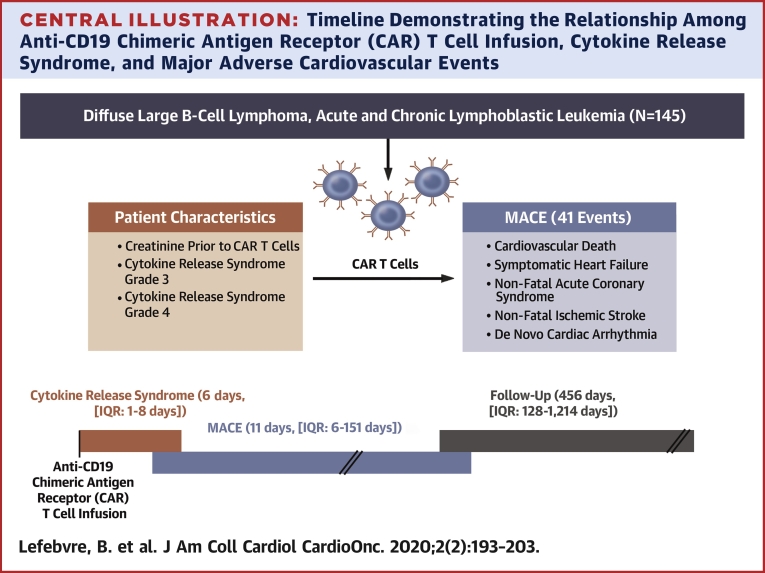
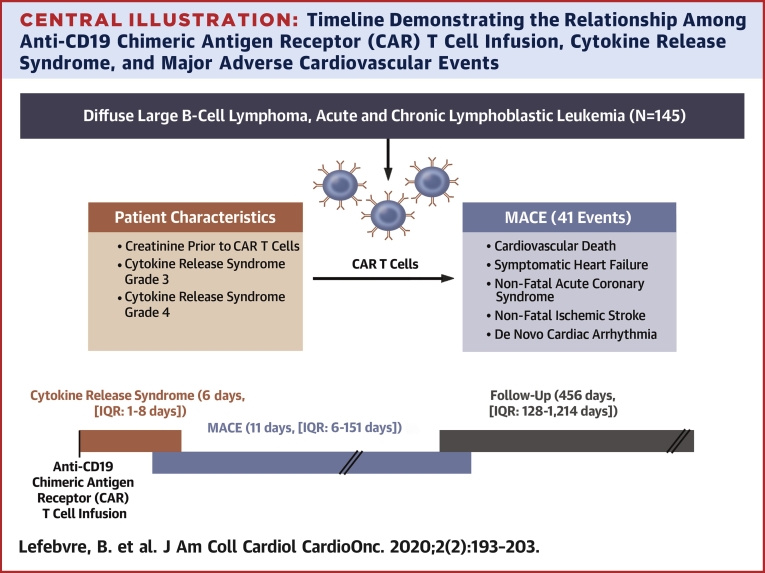
Methods: Baseline clinical, laboratory and echocardiographic parameters were collected in 145 adult patients undergoing CART19 cell therapy. MACE included cardiovascular death, symptomatic heart failure, acute coronary syndrome, ischemic stroke and de novo cardiac arrhythmia. Baseline parameters associated with MACE were identified using Cox proportional cause-specific hazards regression analysis.
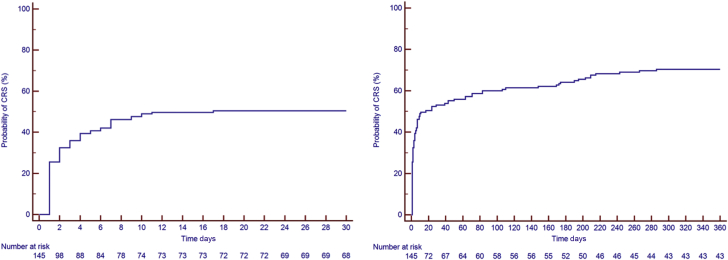
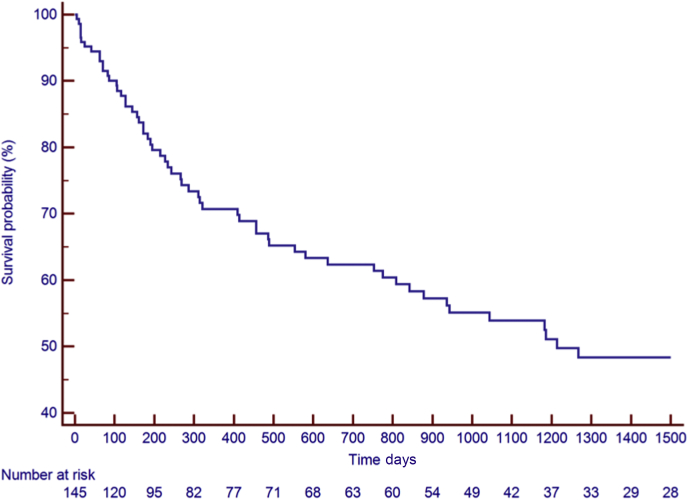
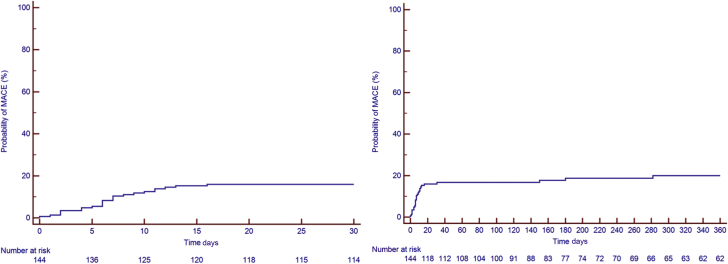
Results: Thirty-one patients had MACE (41 events) at a median time of 11 days (Q1-Q3:6-151 days) after CART19 cell infusion. The median follow-up period was 456 days (Q1-Q3: 128-1214 days). Sixty-one patients died. Cytokine release syndrome (CRS) occurred 176 times in 104 patients; the median time to CRS was 6 days (Q1-Q3: 1-8 days). The Kaplan-Meier estimates for MACE and CRS at 30 days were 17% and 53% respectively. The KM estimates for survival at 1 year was 71%. Multivariable Cox proportional cause-specific hazards regression analysis determined that baseline creatinine and Grade 3 or 4 CRS were independently associated with MACE.
Conclusion: Patients treated with CART19 are at an increased risk of MACE and may benefit from cardiovascular surveillance. Further large prospective studies are needed to confirm the incidence and risk factors predictive of MACE.
Keywords: CART cells; Cardio-oncology; Cardiovascular.
Conflict of interest statement
Declaration of interest : The authors declare no conflicts of interest and have no industry relations to disclose.
Figures
Comment in
-
Cytokines Are at the Heart of It: Cytokine Release Syndrome Underlies Cardiovascular Effects of CAR T Cell.JACC CardioOncol. 2020 Jun 16;2(2):204-206. doi: 10.1016/j.jaccao.2020.05.006. eCollection 2020 Jun. JACC CardioOncol. 2020. PMID: 34396229 Free PMC article.
References
-
- Burstein D.S., Maude S., Grupp S., Griffis H., Rossano J., Lin K. Cardiac profile of chimeric antigen receptor T cell therapy in children: a single-institution experience. Biol Blood Marrow Transplant. 2018;24:1590–1595. - PubMed
-
- Schuster S.J., Bishop M.R., Tam C.S. Tisagenlecleucel in adult relapsed or refractory diffuse large B-cell lymphoma. N Engl J Med. 2019;380:45–56. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
