

Spontaneous Rupture in a Non-Laboring Uterus at 20 Weeks: A Case Report
- PMID: 32776917
- PMCID: PMC7440747
- DOI: 10.12659/AJCR.924894
Spontaneous Rupture in a Non-Laboring Uterus at 20 Weeks: A Case Report
Abstract
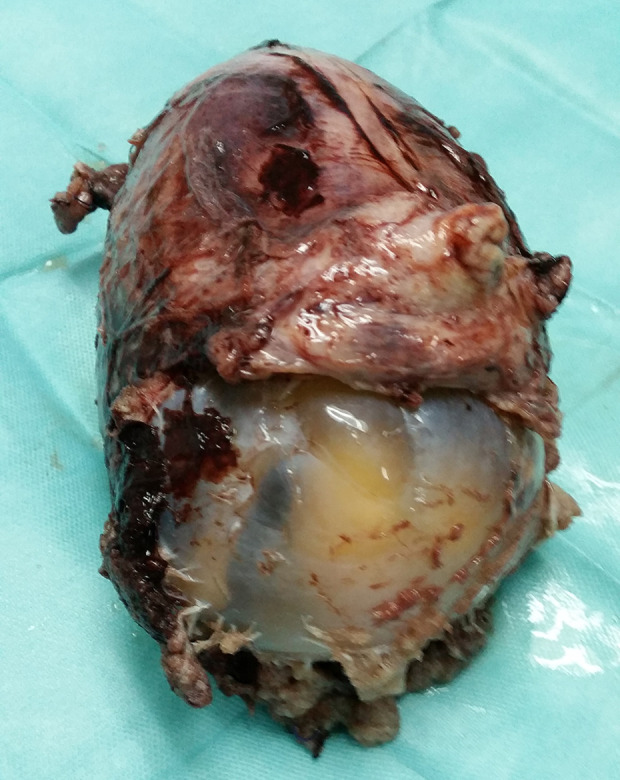
BACKGROUND Uterine rupture is uncommon but when it happens, it can cause significant morbidity and mortality to both mother and fetus. Incidence reportedly is higher in scarred than in unscarred uteri. Most cases occur in laboring women in their third trimester with a previous history of uterine surgery, such as caesarean delivery or myomectomy. We present a case of spontaneous uterine rupture in a non-laboring uterus in the mid-trimester of pregnancy. CASE REPORT The patient presented with threatened miscarriage at 17 weeks' gestation and ultrasound findings were that raised suspicion of a morbidly adherent placenta. Her history was significant for two previous cesarean deliveries more than 5 years ago followed by two spontaneous complete miscarriages in the first trimester. The patient was managed conservatively until 20 weeks' gestation, when she presented with acute abdomen with hypotensive shock. Her hemoglobin dropped to a level such that she required blood transfusion. An emergency exploratory laparotomy was performed, which revealed a 5-cm rupture in the lower part of the anterior wall of the uterus, out of which there was extrusion of part of the placenta. Given the patient's massive bleeding, the decision was made to proceed with subtotal hysterectomy. Histopathology of the specimen confirmed the diagnosis of placenta percreta. CONCLUSIONS Identification of uterine scarring with morbidly adherent placenta is crucial because even in early pregnancy, it can lead to uterine rupture. Furthermore, failure to recognize and promptly manage uterine rupture may prove fatal.
Conflict of interest statement
Figures

Similar articles
-
Placenta percreta with spontaneous rupture of an unscarred uterus in the second trimester.Obstet Gynecol. 2001 Nov;98(5 Pt 2):927-9. doi: 10.1016/s0029-7844(01)01580-0. Obstet Gynecol. 2001. PMID: 11704207
-
Spontaneous rupture of unscarred uterus in the early second trimester: a case report of placenta percreta.Ginekol Pol. 2012 Aug;83(8):626-9. Ginekol Pol. 2012. PMID: 23342889
-
Spontaneous rupture of an unscarred uterus at the early third trimester due to placenta percreta: a case report.J Int Med Res. 2024 Oct;52(10):3000605241281688. doi: 10.1177/03000605241281688. J Int Med Res. 2024. PMID: 39397440 Free PMC article.
-
Uterine preservation in placenta percreta complicated by unscarred uterine rupture at second trimester in a patient with repeated molar pregnancies: a case report and brief review of the literature.Clin Exp Obstet Gynecol. 2014;41(5):590-2. Clin Exp Obstet Gynecol. 2014. PMID: 25864268 Review.
-
Placenta percreta with concomitant uterine didelphys at 18 weeks of pregnancy: a case report and review of the literature.J Matern Fetal Neonatal Med. 2016 Nov;29(21):3445-8. doi: 10.3109/14767058.2015.1130819. Epub 2016 Jan 14. J Matern Fetal Neonatal Med. 2016. PMID: 26653847 Review.
References
-
- Zwart JJ, Richters JM, Ory F, et al. Uterine rupture in The Netherlands: A nationwide population-based cohort study. BJOG. 2009;116(8):1069–78. ; discussion 1078–80. - PubMed
-
- Peker N, Aydin E, Evsen MS, et al. Unscarred uterine rupture and subsequent pregnancy outcome – a tertiary centre experience. Ginekol Pol. 2020;91(2):95–90. - PubMed
-
- Kaczmarczyk M, Sparen P, Terry P, Cnattingius S. Risk factors for uterine rupture and neonatal consequences of uterine rupture: A population-based study of successive pregnancies in Sweden. BJOG. 2007;114(10):1208–14. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
