

Practice Patterns and Responsiveness to Simulated Common Ocular Complaints Among US Ophthalmology Centers During the COVID-19 Pandemic
- PMID: 32777008
- PMCID: PMC7407319
- DOI: 10.1001/jamaophthalmol.2020.3237
Practice Patterns and Responsiveness to Simulated Common Ocular Complaints Among US Ophthalmology Centers During the COVID-19 Pandemic
Abstract
Importance: The coronavirus disease 2019 (COVID-19) pandemic has drastically changed how comprehensive ophthalmology practices care for patients.
Objective: To report practice patterns for common ocular complaints during the initial stage of the COVID-19 pandemic among comprehensive ophthalmology practices in the US.
Design, setting, and participants: In this cross-sectional study, 40 private practices and 20 university centers were randomly selected from 4 regions across the US. Data were collected on April 29 and 30, 2020.
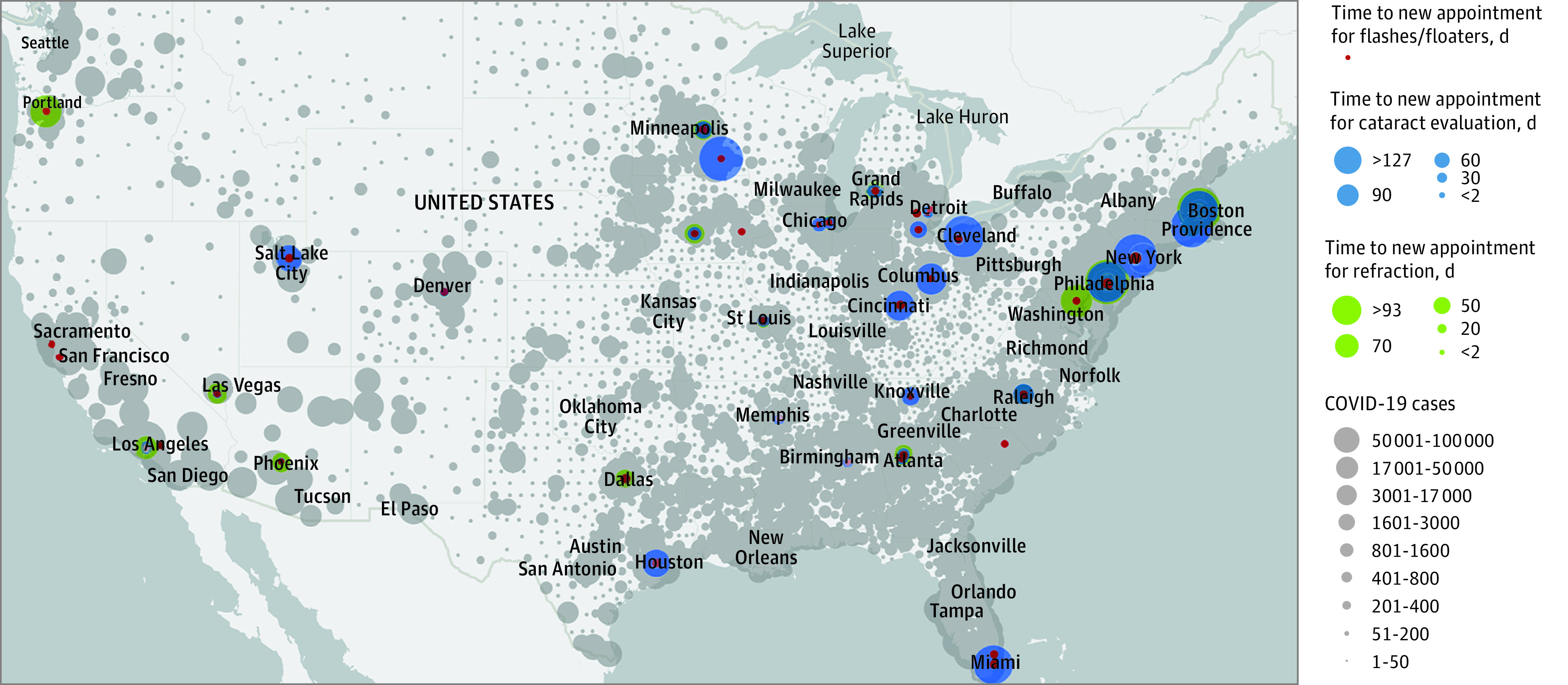
Interventions: Investigators placed telephone calls to each ophthalmology practice office. Responses to 3 clinical scenarios-refraction request, cataract evaluation, and symptoms of a posterior vitreous detachment-were compared regionally and between private and university centers.
Main outcomes and measures: The primary measure was time to next appointment for each of the 3 scenarios. Secondary measures included use of telemedicine and advertisement of COVID-19 precautions.
Results: Of the 40 private practices, 2 (5%) were closed, 24 (60%) were only seeing urgent patients, and 14 (35%) remained open to all patients. Of the 20 university centers, 2 (10%) were closed, 17 (85%) were only seeing urgent patients, and 1 (5%) remained open to all patients. There were no differences for any telemedicine metric. University centers were more likely than private practices to mention preparations to limit the spread of COVID-19 (17 of 20 [85%] vs 14 of 40 [35%]; mean difference, 0.41; 95% CI, 0.26-0.65; P < .001). Private practices had a faster next available appointment for cataract evaluations than university centers, with a mean (SD) time to visit of 22.1 (27.0) days vs 75.5 (46.1) days (mean difference, 53.4; 95% CI, 23.1-83.7; P < .001). Private practices were also more likely than university centers to be available to see patients with flashes and floaters (30 of 40 [75%] vs 8 of 20 [40%]; mean difference, 0.42; 95% CI, 0.22-0.79; P = .01).
Conclusions and relevance: In this cross-sectional study of investigator telephone calls to ophthalmology practice offices, there were uniform recommendations for the 3 routine ophthalmic complaints. Private practices had shorter times to next available appointment for cataract extraction and were more likely to evaluate posterior vitreous detachment symptoms. As there has not been a study examining these practice patterns before the COVID-19 pandemic, the relevance of these findings on public health is yet to be determined.
Conflict of interest statement
Figures
Comment in
-
Insights Into Eye Care Practice During COVID-19.JAMA Ophthalmol. 2020 Sep 1;138(9):988-989. doi: 10.1001/jamaophthalmol.2020.3244. JAMA Ophthalmol. 2020. PMID: 32777017 No abstract available.
References
-
- American College of Surgeons COVID-19: recommendations for management of elective surgical procedures. Accessed May 3, 2020. https://www.facs.org/covid-19/clinical-guidance/elective-surgery
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
