

Endovascular Treatment After Stroke Due to Large Vessel Occlusion for Patients Presenting Very Late From Time Last Known Well
- PMID: 32777014
- PMCID: PMC7418043
- DOI: 10.1001/jamaneurol.2020.2804
Endovascular Treatment After Stroke Due to Large Vessel Occlusion for Patients Presenting Very Late From Time Last Known Well
Abstract
Importance: Endovascular treatment (EVT) after ischemic stroke due to emergent large vessel occlusion is usually constrained by a specific window of less than 16 to 24 hours from the time the patient was last known well (LKW). Patients with slow progression and tenacious collateral circulation may persist beyond 16 hours.
Objectives: To estimate the prevalence of salvageable tissues 16 hours or more from LKW after ischemic stroke due to emergent large vessel occlusion and investigate the effectiveness of EVT in delayed large vessel occlusion.
Design, setting and participants: In this case-control study, from a total of 8032 patients with stroke or transient ischemic attack who were admitted between January 1, 2012, and December 31, 2018, to a single referral university hospital, 150 patients were retrospectively identified who had an acute ischemic stroke with internal carotid artery or middle cerebral artery occlusion, had a baseline National Institutes of Health Stroke Scale score of 6 or more, and arrived 16 hours or more from time LKW. The decision for EVT was made by a treating physician according to the institutional protocol.
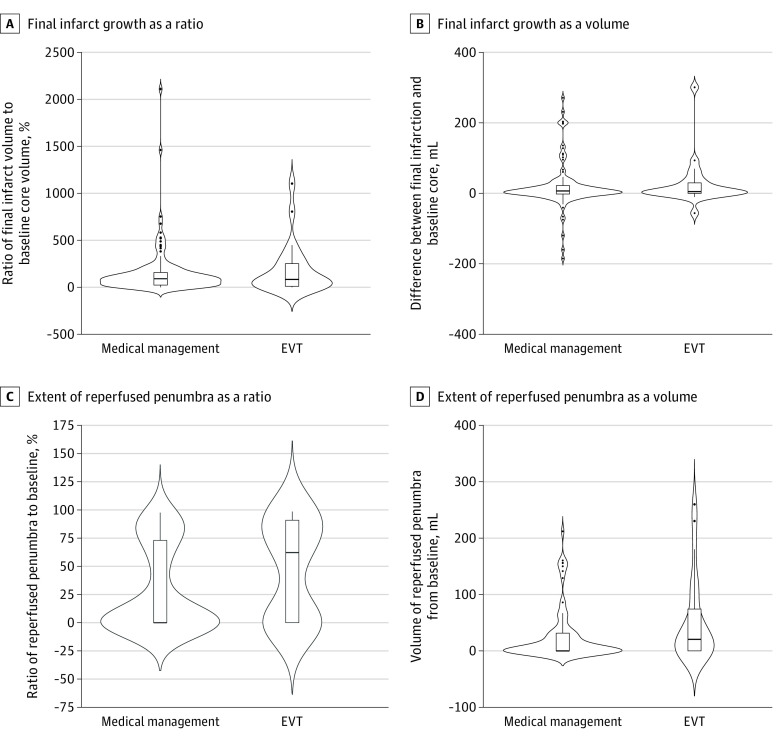
Main outcomes and measures: Baseline ischemic core, collateral circulation status, and computed tomographic or magnetic resonance perfusion parameters were retrospectively quantified. Follow-up images, evaluated a median of 93 hours (interquartile range, 66-120 hours) after arrival, were used to assess the final infarct and hemorrhagic transformation. The main outcome was the modified Rankin Scale score at 90 days.
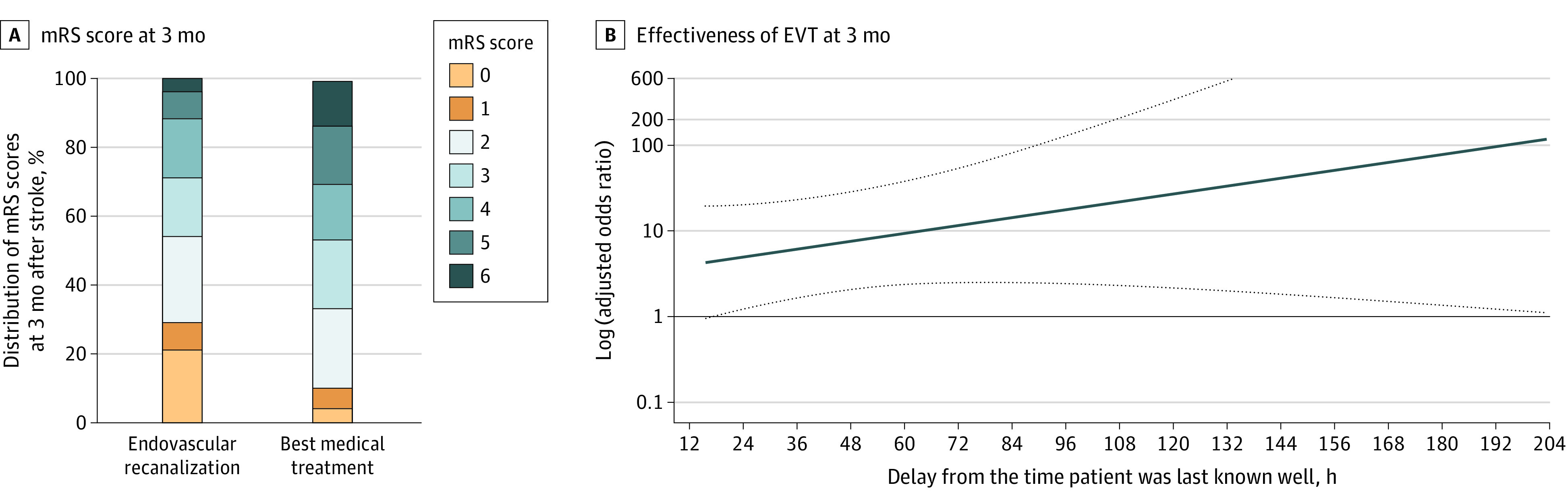
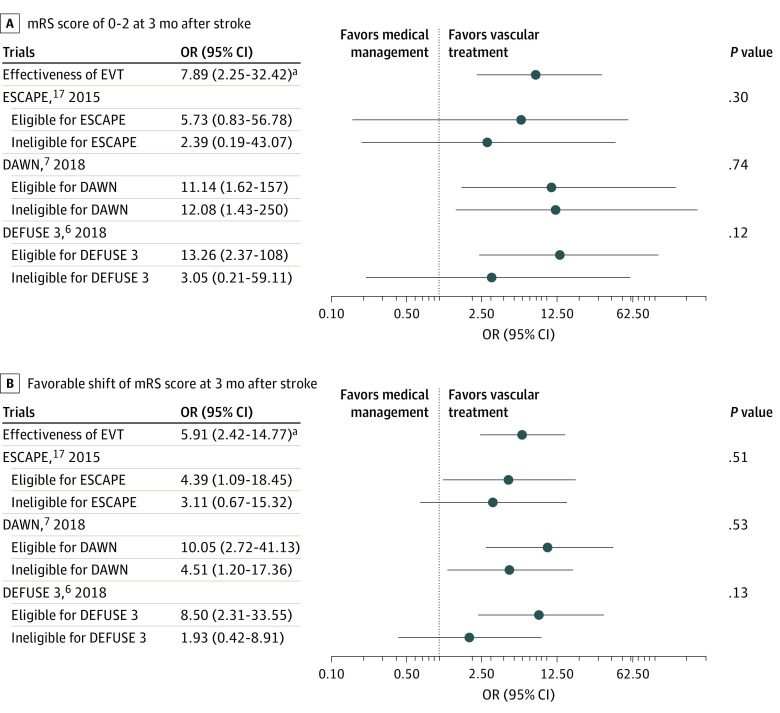
Results: For 150 patients (81 men [54%]; mean [SD] age at onset, 70.1 [13.0] years; median National Institutes of Health Stroke Scale score, 12 [interquartile range, 8-18]), the median ischemic core volume was 11.5 mL (interquartile range, 0-39.1 mL), the median penumbra volume (>6 seconds) was 55.0 mL (interquartile range, 15-128 mL), and the median mismatch ratio was 4.0 (interquartile range, 0.9-18.3). By the imaging inclusion criteria for EVT trials, there were 50 DAWN (DWI or CTP Assessment With Clinical Mismatch in the Triage of Wake-up and Late Presenting Strokes Undergoing Neurointervention With Trevo)-eligible patients (33%), 58 DEFUSE 3 (Endovascular Therapy Following Imaging Evaluation for Ischemic Stroke)-eligible patients (39%), and 57 ESCAPE (Endovascular Treatment for Small Core and Anterior Circulation Proximal Occlusion With Emphasis on Minimizing CT to Recanalization Times)-eligible patients (38%). Endovascular treatment was performed for 24 patients (16%). In propensity score-matched analyses, EVT was associated with better odds of a 90-day modified Rankin Scale score of 0 to 2 (adjusted odds ratio, 11.08 [95% CI, 1.88-108.60]) and a 90-day modified Rankin Scale score shift (common adjusted odds ratio, 5.17 [95% CI, 1.80-15.62]). Type 2 parenchymal hemorrhage was seen in 3 of 24 patients (13%) who received EVT and in 4 of 126 patients (3%) who received medical management (adjusted odds ratio, 4.06 [95% CI, 0.63-26.30]). In a subgroup of 109 patients who were 24 hours from time LKW, EVT was associated with a favorable mRS shift (common adjusted odds ratio, 10.54 [95% CI, 2.18-59.34]).
Conclusions and relevance: This study suggests that patients with anterior circulation large vessel occlusion presenting very late (>16 hours to 10 days) from the time they were LKW may benefit from EVT.
Conflict of interest statement
Figures
References
-
- Powers WJ, Rabinstein AA, Ackerson T, et al. Guidelines for the early management of patients with acute ischemic stroke: 2019 update to the 2018 guidelines for the early management of acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2019;50(12):e344-e418. doi: 10.1161/STR.0000000000000211 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
