

Comparison of Heart Team vs Interventional Cardiologist Recommendations for the Treatment of Patients With Multivessel Coronary Artery Disease
- PMID: 32777060
- PMCID: PMC7417969
- DOI: 10.1001/jamanetworkopen.2020.12749
Comparison of Heart Team vs Interventional Cardiologist Recommendations for the Treatment of Patients With Multivessel Coronary Artery Disease
Abstract
Importance: Although the heart team approach is recommended in revascularization guidelines, the frequency with which heart team decisions differ from those of the original treating interventional cardiologist is unknown.
Objective: To examine the difference in decisions between the heart team and the original treating interventional cardiologist for the treatment of patients with multivessel coronary artery disease.
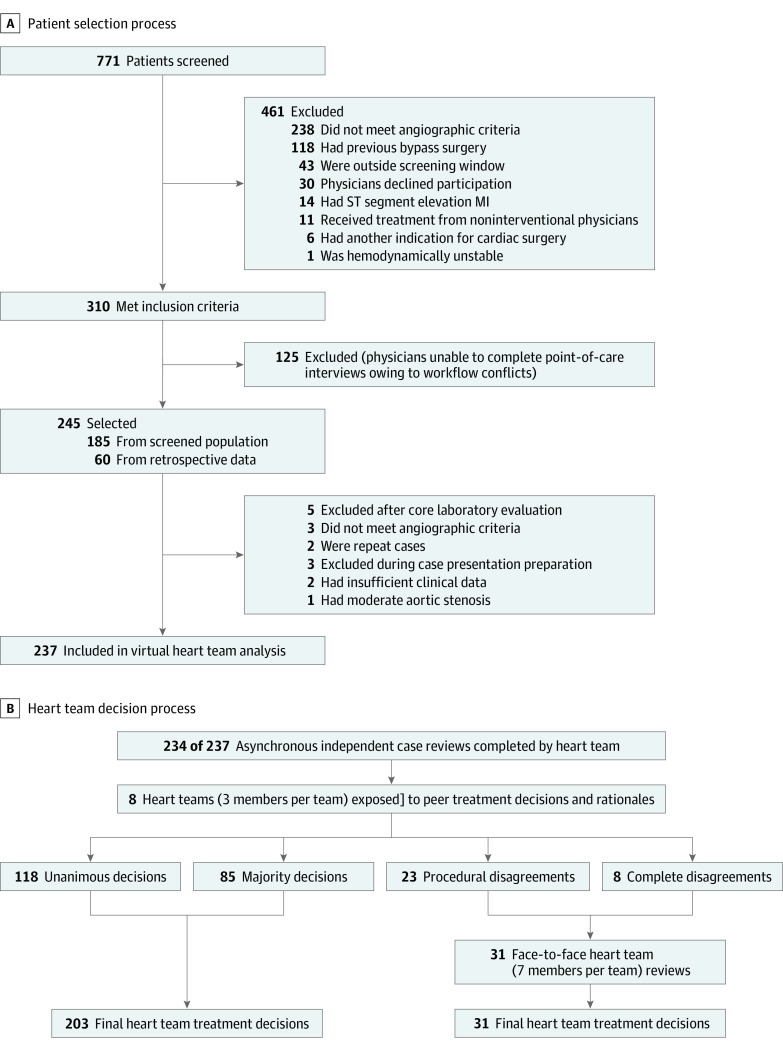
Design, setting, and participants: In this cross-sectional study, 245 consecutive patients with multivessel coronary artery disease were recruited from 1 high-volume tertiary care referral center (185 patients were enrolled through a screening process, and 60 patients were retrospectively enrolled from the center's database). A total of 237 patients were included in the final virtual heart team analysis. Treatment decisions (which comprised coronary artery bypass grafting, percutaneous coronary intervention, and medication therapy) were made by the original treating interventional cardiologists between March 15, 2012, and October 20, 2014. These decisions were then compared with pooled-majority treatment decisions made by 8 blinded heart teams using structured online case presentations between October 1, 2017, and October 15, 2018. The randomized members of the heart teams comprised experts from 3 domains, with each team containing 1 noninvasive cardiologist, 1 interventional cardiologist, and 1 cardiovascular surgeon. Cases in which all 3 of the heart team members disagreed and cases in which procedural discordance occurred (eg, 2 members chose coronary artery bypass grafting and 1 member chose percutaneous coronary intervention) were discussed in a face-to-face heart team review in October 2018 to obtain pooled-majority decisions. Data were analyzed from May 6, 2019, to April 22, 2020.
Main outcomes and measures: The Cohen κ coefficient between the treatment recommendation from the heart team and the treatment recommendation from the original treating interventional cardiologist.
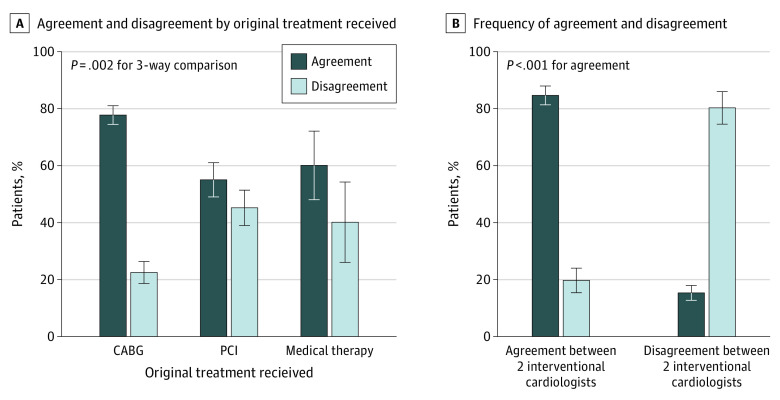
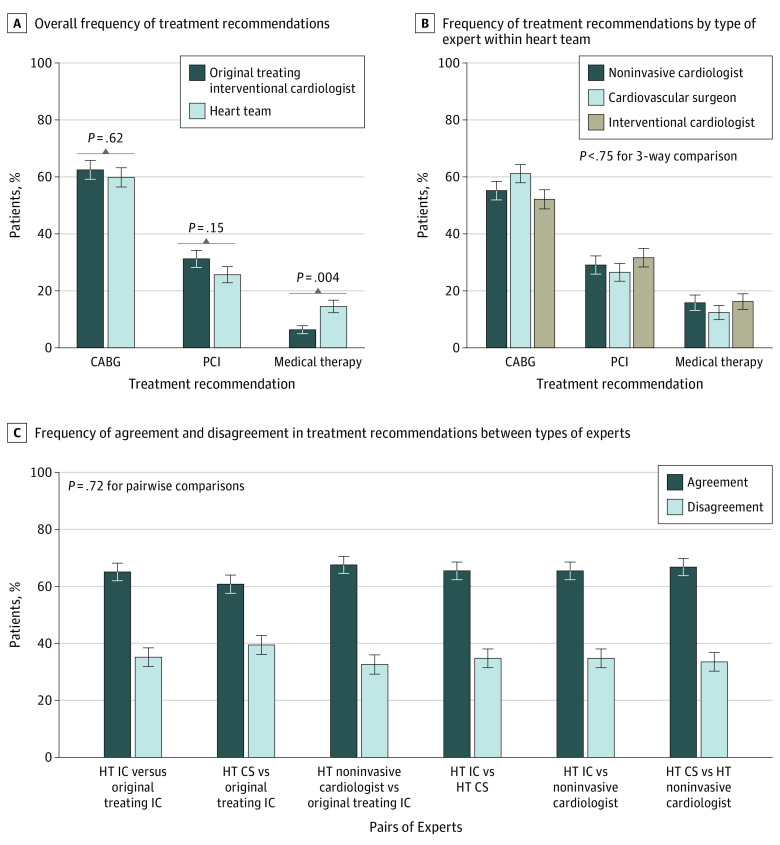
Results: Among 234 of 237 patients (98.7%) in the analysis for whom complete data were available, the mean (SD) age was 67.8 (10.9) years; 176 patients (75.2%) were male, and 191 patients (81.4%) had stenosis in 3 epicardial coronary vessels. A total of 71 differences (30.3%; 95% CI, 24.5%-36.7%) in treatment decisions between the heart team and the original treating interventional cardiologist occurred, with a Cohen κ of 0.478 (95% CI, 0.336-0.540; P = .006). The heart team decision was more frequently unanimous when it was concordant with the decision of the original treating interventional cardiologist (109 of 163 cases [66.9%]) compared with when it was discordant (28 of 71 cases [39.4%]; P < .001). When the heart team agreed with the original treatment decision, there was more agreement between the heart team interventional cardiologist and the original treating interventional cardiologist (138 of 163 cases [84.7%]) compared with when the heart team disagreed with the original treatment decision (14 of 71 cases [19.7%]); P < .001). Those with an original treatment of coronary artery bypass grafting, percutaneous coronary intervention, and medication therapy, 32 of 148 patients [22.3%], 32 of 71 patients [45.1%], and 6 of 15 patients [40.0%], respectively, received a different treatment recommendation from the heart team than the original treating interventional cardiologist; the difference across the 3 groups was statistically significant (P = .002).
Conclusions and relevance: The heart team's recommended treatment for patients with multivessel coronary artery disease differed from that of the original treating interventional cardiologist in up to 30% of cases. This subset of cases was associated with a lower frequency of unanimous decisions within the heart team and less concordance between the interventional cardiologists; discordance was more frequent when percutaneous coronary intervention or medication therapy were considered. Further research is needed to evaluate whether heart team decisions are associated with improvements in outcomes and, if so, how to identify patients for whom the heart team approach would be beneficial.
Conflict of interest statement
Figures
Comment in
-
Treatment Recommendations for Patients With Multivessel Coronary Artery Disease-There Is No "I" in Heart Team, But Is the Heart Team Better Than the I?JAMA Netw Open. 2020 Aug 3;3(8):e2013098. doi: 10.1001/jamanetworkopen.2020.13098. JAMA Netw Open. 2020. PMID: 32777057 No abstract available.
References
-
- Teo KK, Cohen E, Buller C, et al. . Canadian Cardiovascular Society/Canadian Association of Interventional Cardiology/Canadian Society of Cardiac Surgery position statement on revascularization—multivessel coronary artery disease. Can J Cardiol. 2014;30(12):1482-1491. doi:10.1016/j.cjca.2014.09.034 - DOI - PubMed
-
- Fihn SD, Blankenship JC, Alexander KP, et al. . 2014 ACC/AHA/AATS/PCNA/SCAI/STS focused update of the guideline for the diagnosis and management of patients with stable ischemic heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines, and the American Association for Thoracic Surgery, Preventive Cardiovascular Nurses Association, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. J Am Coll Cardiol. 2014;64(18):1929-1949. doi:10.1016/j.jacc.2014.07.017 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
