

Perioperative non-invasive versus semi-invasive cardiac index monitoring in patients with bariatric surgery - a prospective observational study
- PMID: 32778047
- PMCID: PMC7419223
- DOI: 10.1186/s12871-020-01110-x
Perioperative non-invasive versus semi-invasive cardiac index monitoring in patients with bariatric surgery - a prospective observational study
Abstract
Background: In morbidly obese patients undergoing laparoscopic bariatric surgery, the combination of obesity-related comorbidities, pneumoperitoneum and extreme posture changes constitutes a high risk of perioperative hemodynamic complications. Thus, an advanced hemodynamic monitoring including continuous cardiac index (CI) assessment is desirable. While invasive catheterization may bear technical difficulties, transesophageal echocardiography is contraindicated due to the surgical procedure. Evidence on the clinical reliability of alternative semi- or non-invasive cardiac monitoring devices is limited. The aim was to compare the non-invasive vascular unloading to a semi-invasive pulse contour analysis reference technique for continuous CI measurements in bariatric surgical patients.
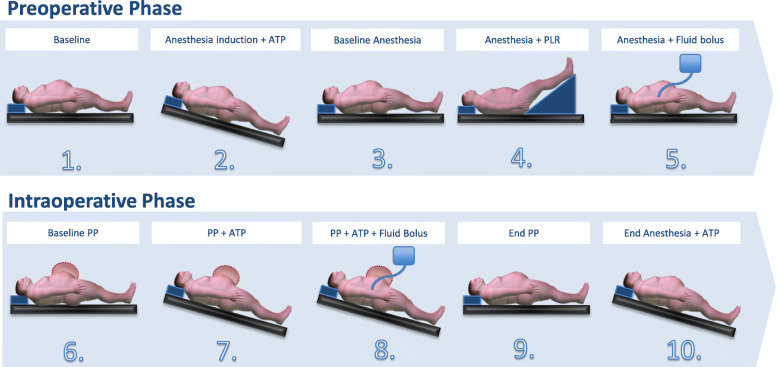
Methods: This prospective observational study included adult patients scheduled for elective, laparoscopic bariatric surgery after obtained institutional ethics approval and written informed consent. CI measurements were performed using the vascular unloading technique (Nexfin®) and semi-invasive reference method (FloTrac™). At 10 defined measurement time points, the influence of clinically indicated body posture changes, passive leg raising, fluid bolus administration and pneumoperitoneum was evaluated pre- and intraoperatively. Correlation, Bland-Altman and concordance analyses were performed.
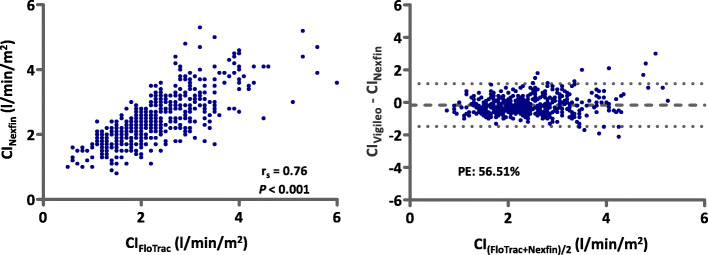
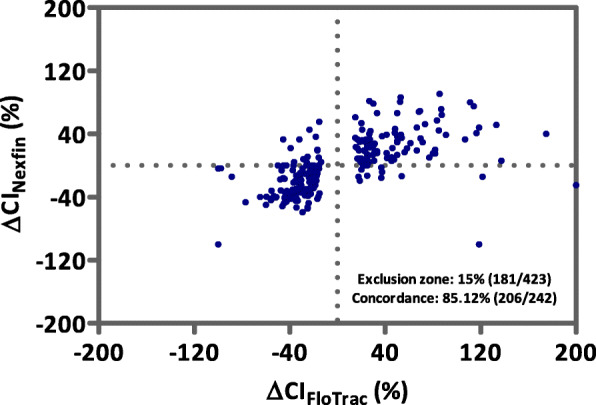
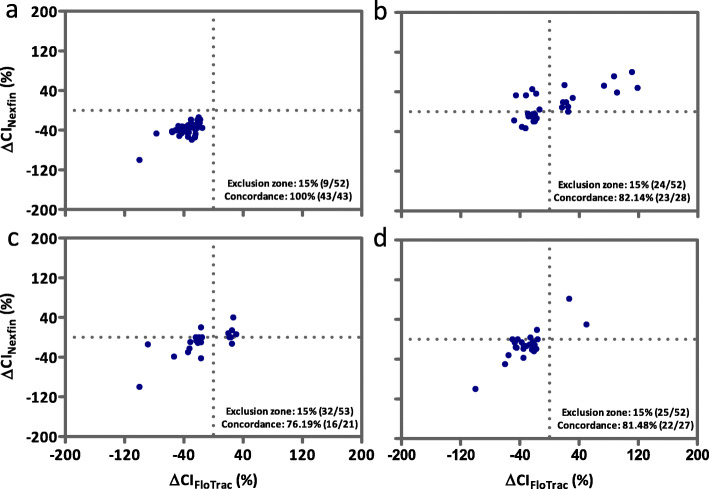
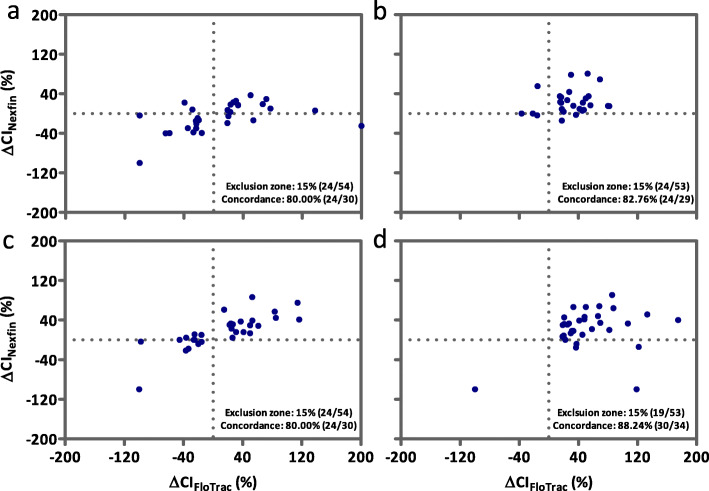
Results: Sixty patients (mean BMI 49.2 kg/m2) were enrolled into the study and data from 54 patients could be entered in the final analysis. Baseline CI was 3.2 ± 0.9 and 3.3 ± 0.8 l/min/m2, respectively. Pooled absolute CI values showed a positive correlation (rs = 0.76, P < 0.001) and mean bias of of - 0.16 l/min/m2 (limits of agreement: - 1.48 to 1.15 l/min/m2) between the two methods. Pooled percentage error was 56.51%, missing the criteria of interchangeability (< 30%). Preoperatively, bias ranged from - 0.33 to 0.08 l/min/m2 with wide limits of agreement. Correlation of CI was best (rs = 0.82, P < 0.001) and percentage error lowest (46.34%) during anesthesia and after fluid bolus administration. Intraoperatively, bias ranged from - 0.34 to - 0.03 l/min/m2 with wide limits of agreement. CI measurements correlated best during pneumoperitoneum and after fluid bolus administration (rs = 0.77, P < 0.001; percentage error 35.95%). Trending ability for all 10 measurement points showed a concordance rate of 85.12%, not reaching the predefined Critchley criterion (> 92%).
Conclusion: Non-invasive as compared to semi-invasive CI measurements did not reach criteria of interchangeability for monitoring absolute and trending values of CI in morbidly obese patients undergoing bariatric surgery.
Trial registration: The study was registered retrospectively on June 12, 2017 with the registration number NCT03184272 .
Keywords: Bariatric surgery; Cardiac output; Finger-cuff; Hemodynamic monitoring; Non-invasive monitoring; Obesity; Vascular unloading technique.
Conflict of interest statement
All authors have provided information on potential conflicts of interests directly or indirectly related to the work submitted. All other authors declared that they have no conflict of interest.
Figures
References
-
- Angrisani L, Santonicola A, Iovino P, Formisano G, Buchwald H, Scopinaro N. Bariatric surgery worldwide 2013. Obes Surg. 2015;25:1822–1832. - PubMed
-
- Fried M, Yumuk V, Oppert JM, Scopinaro N, Torres AJ, Weiner R, Yashkov Y, Fruhbeck G, European Association for the Study of O, International Federation for the Surgery of Obesity - European C Interdisciplinary European guidelines on metabolic and bariatric surgery. Obes Facts. 2013;6:449–468. - PMC - PubMed
-
- Kaya C, Bilgin S, Cebeci GC, Tomak L. Anaesthetic management of patients undergoing bariatric surgery. J Coll Physicians Surg Pak. 2019;29:757–762. - PubMed
-
- Tsai A, Schumann R. Morbid obesity and perioperative complications. Curr Opin Anaesthesiol. 2016;29:103–108. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
