

Effects of Epeleuton, a Novel Synthetic Second-Generation n-3 Fatty Acid, on Non-Alcoholic Fatty Liver Disease, Triglycerides, Glycemic Control, and Cardiometabolic and Inflammatory Markers
- PMID: 32779505
- PMCID: PMC7660824
- DOI: 10.1161/JAHA.119.016334
Effects of Epeleuton, a Novel Synthetic Second-Generation n-3 Fatty Acid, on Non-Alcoholic Fatty Liver Disease, Triglycerides, Glycemic Control, and Cardiometabolic and Inflammatory Markers
Abstract
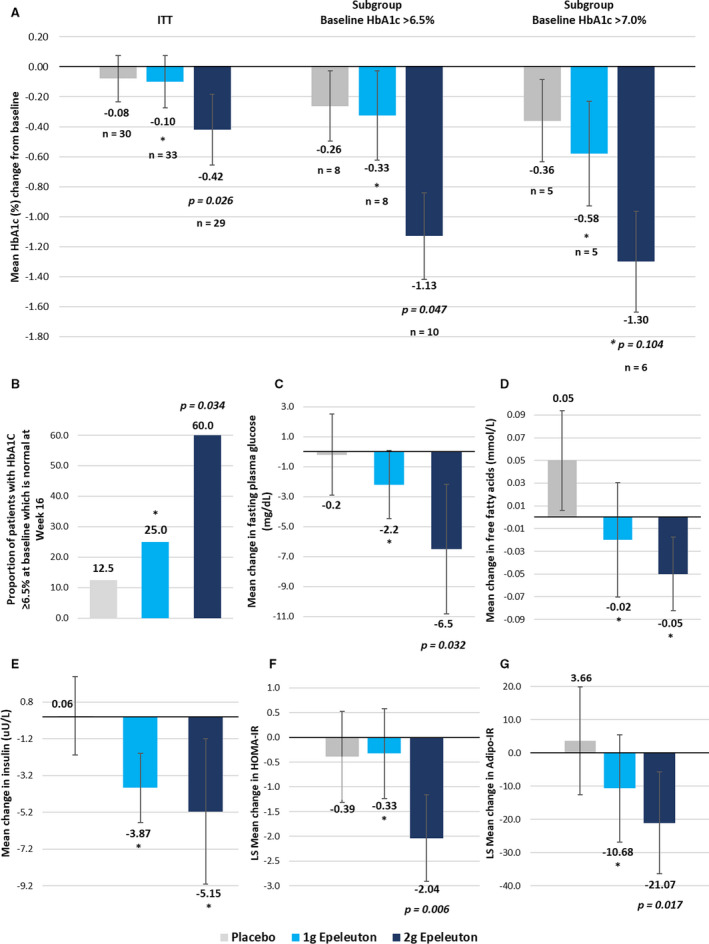
Background Epeleuton is 15-hydroxy eicosapentaenoic acid ethyl ester, a second-generation synthetic n-3 fatty acid derivative of eicosapentaenoic acid. The primary objective was to assess the effect of epeleuton on markers of nonalcoholic fatty liver disease (NAFLD) with post hoc analyses of cardiometabolic markers. Methods and Results In a multicenter, randomized, double-blind, placebo-controlled trial, 96 adults with nonalcoholic fatty liver disease and body mass index 25 to 40 were randomized in a 1:1:1 ratio to receive epeleuton 2 g/day, epeleuton 1 g/day, or placebo for 16 weeks. A total of 27% of patients had diabetes mellitus. Primary end points of changes in alanine aminotransferase and liver stiffness did not improve at week 16. Secondary and post hoc analyses investigated changes in cardiometabolic markers. Epeleuton 2 g/day significantly decreased triglycerides, very-low-density lipoprotein cholesterol, and total cholesterol without increasing low-density lipoprotein cholesterol. Despite a low mean baseline hemoglobin A1C (HbA1C; 6.3±1.3%), epeleuton 2 g/day significantly decreased HbA1c (-0.4%; P=0.026). Among patients with baseline HbA1c >6.5%, epeleuton 2 g/day decreased HbA1c by 1.1% (P=0.047; n=26). Consistent dose-dependent reductions were observed for fasting plasma glucose, insulin, and insulin resistance indices. Epeleuton 2 g/day decreased circulating markers of cardiovascular risk and endothelial dysfunction. Epeleuton was well tolerated, with a safety profile not different from placebo. Conclusions While epeleuton did not meet its primary end points on alanine aminotransferase or liver stiffness, it significantly decreased triglycerides, HbA1C, plasma glucose, and inflammatory markers. These data suggest epeleuton may have potential for cardiovascular risk reduction and nonalcoholic fatty liver disease by simultaneously targeting hypertriglyceridemia, hyperglycemia, and systemic inflammation. Further trials are planned. Registration URL: https://www.clinicaltrials.gov; Unique identifier: NCT02941549.
Keywords: 15‐HEPE; DS102; epeleuton; n‐3 fatty acid.
Conflict of interest statement
Dr Climax is the CEO and a shareholder of Afimmune and DS Biopharma. Dr Newsome has received grants, consultancy, and nonfinancial support from Novo Nordisk; consultancy from Shire; grants and consultancy from Boehringer Ingelheim; consultancy from Intercept Pharmaceuticals; consultancy from Afimmune; speaker fees from Norgine; consultancy from Gilead Sciences; and consultancy from Pfizer. Drs Hamza, Weissbach, and Coughlan are employees of Afimmune and DS Biopharma. Dr Sattar has consulted for, or received speaker fees from, Afimmune, Amgen, Boehringer Ingelheim, AstraZeneca, Eli Lilly, Novo Nordisk, Sanofi, and Janssen and has received research grant support from Boehringer Ingelheim. Dr McGuire has received honoraria for clinical trial leadership from AstraZeneca, Sanofi Aventis, Janssen, Boehringer Ingelheim, Merck & Co, Pfizer, Novo Nordisk, Lexicon, Eisai Inc, GlaxoSmithKline, and Esperion and honoraria for consultancy from AstraZeneca, Sanofi Aventis, Eli Lilly and Company, Boehringer Ingelheim, Merck & Co, Pfizer, Novo Nordisk, Metavant, Applied Therapeutics, and Afimmune. Dr Bhatt discloses the following relationships—Advisory Board: Cardax, CellProthera, Cereno Scientific, Elsevier Practice Update Cardiology, Level Ex, Medscape Cardiology, PhaseBio, PLx Pharma, Regado Biosciences; Board of Directors: Boston VA Research Institute, Society of Cardiovascular Patient Care, TobeSoft; Chair: American Heart Association Quality Oversight Committee; Data Monitoring Committees: Baim Institute for Clinical Research (formerly Harvard Clinical Research Institute, for the PORTICO trial, funded by St. Jude Medical, now Abbott), Cleveland Clinic (including for the ExCEED trial, funded by Edwards), Contego Medical (Chair, PERFORMANCE 2), Duke Clinical Research Institute, Mayo Clinic, Mount Sinai School of Medicine (for the ENVISAGE trial, funded by Daiichi Sankyo), Population Health Research Institute; Honoraria: American College of Cardiology (Senior Associate Editor, Clinical Trials and News, ACC.org; Vice‐Chair, ACC Accreditation Committee), Baim Institute for Clinical Research (formerly Harvard Clinical Research Institute; RE‐DUAL PCI clinical trial steering committee funded by Boehringer Ingelheim; AEGIS‐II executive committee funded by CSL Behring), Belvoir Publications (Editor in Chief,
Figures


References
-
- Herrington W, Lacey B, Sherliker P, Armitage J, Lewington S. Epidemiology of atherosclerosis and the potential to reduce the global burden of atherothrombotic disease. Circ Res. 2016;535–546. - PubMed
-
- Zelniker TA, Wiviott SD, Raz I, Im K, Goodrich EL, Furtado RHM, Bonaca MP, Mosenzon O, Kato ET, Cahn A, et al. Comparison of the effects of glucagon‐like peptide receptor agonists and sodium‐glucose cotransporter 2 inhibitors for prevention of major adverse cardiovascular and renal outcomes in type 2 diabetes mellitus. Circulation. 2019;2022–2031. - PubMed
-
- Bhatt DL, Steg PG, Miller M, Brinton EA, Jacobson TA, Ketchum SB, Doyle RT, Juliano RA, Jiao L, Granowitz C, et al. Cardiovascular risk reduction with icosapent ethyl for hypertriglyceridemia. N Engl J Med. 2019;11–22. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
