

Definitions and classification of malformations of cortical development: practical guidelines
- PMID: 32779696
- PMCID: PMC7586092
- DOI: 10.1093/brain/awaa174
Definitions and classification of malformations of cortical development: practical guidelines
Erratum in
-
Corrigendum to: Definitions and classification of malformations of cortical development: practical guidelines.Brain. 2020 Dec 1;143(12):e108. doi: 10.1093/brain/awaa298. Brain. 2020. PMID: 32968766 Free PMC article. No abstract available.
Abstract
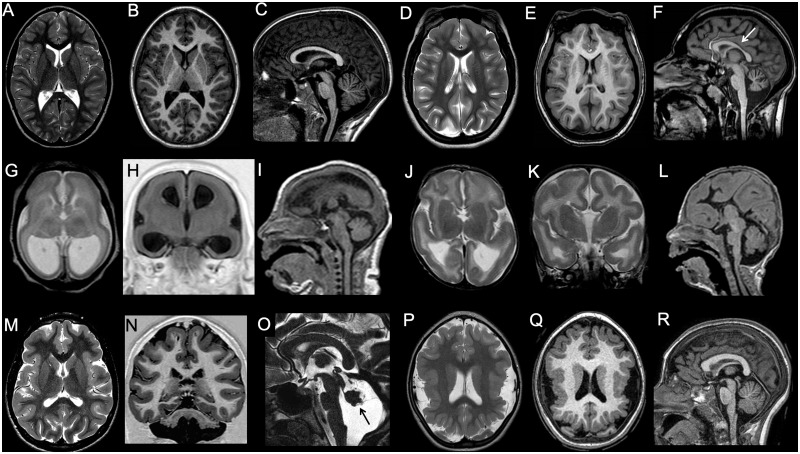
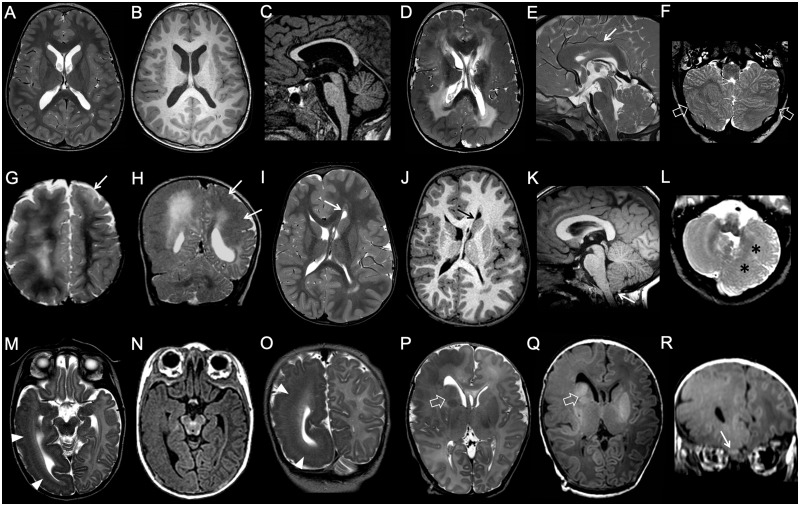
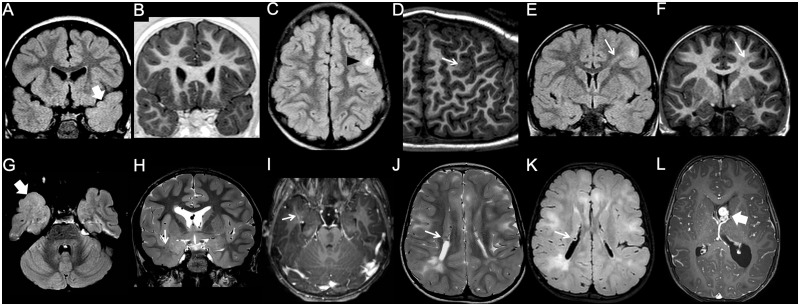
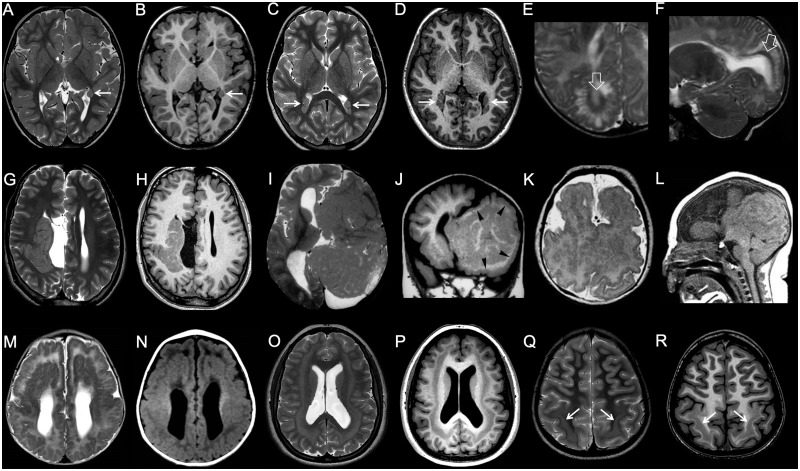
Malformations of cortical development are a group of rare disorders commonly manifesting with developmental delay, cerebral palsy or seizures. The neurological outcome is extremely variable depending on the type, extent and severity of the malformation and the involved genetic pathways of brain development. Neuroimaging plays an essential role in the diagnosis of these malformations, but several issues regarding malformations of cortical development definitions and classification remain unclear. The purpose of this consensus statement is to provide standardized malformations of cortical development terminology and classification for neuroradiological pattern interpretation. A committee of international experts in paediatric neuroradiology prepared systematic literature reviews and formulated neuroimaging recommendations in collaboration with geneticists, paediatric neurologists and pathologists during consensus meetings in the context of the European Network Neuro-MIG initiative on Brain Malformations (https://www.neuro-mig.org/). Malformations of cortical development neuroimaging features and practical recommendations are provided to aid both expert and non-expert radiologists and neurologists who may encounter patients with malformations of cortical development in their practice, with the aim of improving malformations of cortical development diagnosis and imaging interpretation worldwide.
Keywords: classification; epilepsy; malformations of cortical development; neuroimaging.
© The Author(s) (2020). Published by Oxford University Press on behalf of the Guarantors of Brain.
Figures
References
-
- Alcantara D, ÓDriscoll M.. Congenital microcephaly. Am J Med Genet C Genet 2014; 166C: 124–39. - PubMed
-
- Aronica E, Mühlebner A.. Neuropathology of epilepsy. Handb Clin Neurol 2017; 145: 193–216. - PubMed
-
- Ashwal S, Michelson D, Plawner L, Dobyns WB.. Quality Standards Subcommittee of the American Academy of Neurology and the Practice Committee of the Child Neurology Society. Practice parameter: evaluation of the child with microcephaly (an evidence-based review): report of the Quality Standards Subcommittee of the American Academy of Neurology and the Practice Committee of the Child Neurology Society. Neurology 2009; 73: 887–97. - PMC - PubMed
-
- Astick M, Vanderhaeghen P.. From human pluripotent stem cells to cortical circuits. Curr Top Dev Biol 2018; 129: 67–98. - PubMed
