

Anterior Cervical Osteophyte Resection for Treatment of Dysphagia
- PMID: 32779946
- PMCID: PMC8119911
- DOI: 10.1177/2192568220912706
Anterior Cervical Osteophyte Resection for Treatment of Dysphagia
Abstract
Study design: This was a retrospective cohort study.
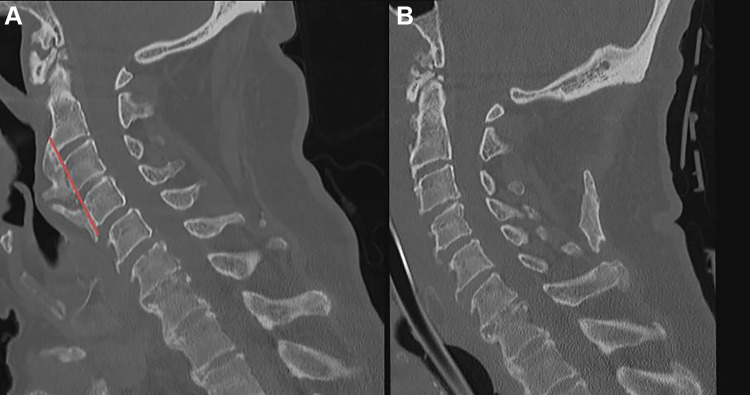
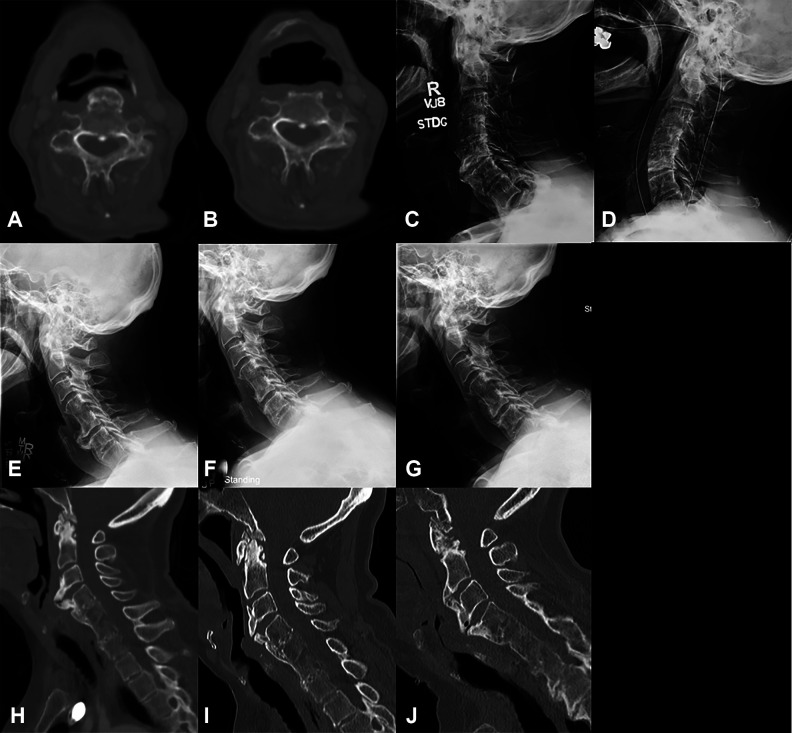
Objectives: When anterior cervical osteophytes become large enough, they may cause dysphagia. There is a paucity of work examining outcomes and complications of anterior cervical osteophyte resection for dysphagia.
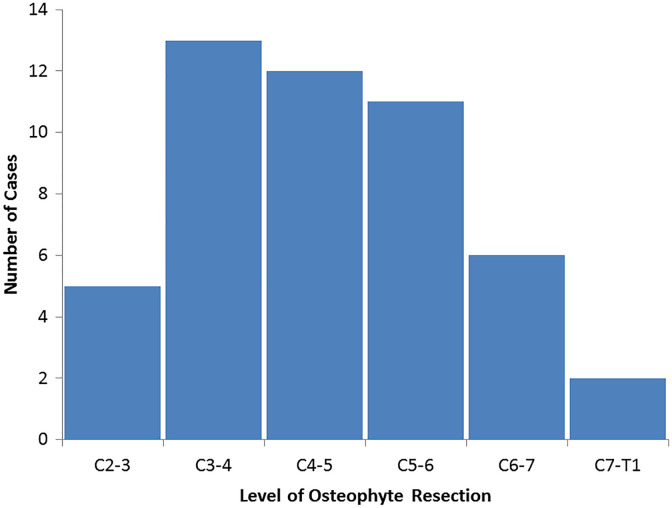
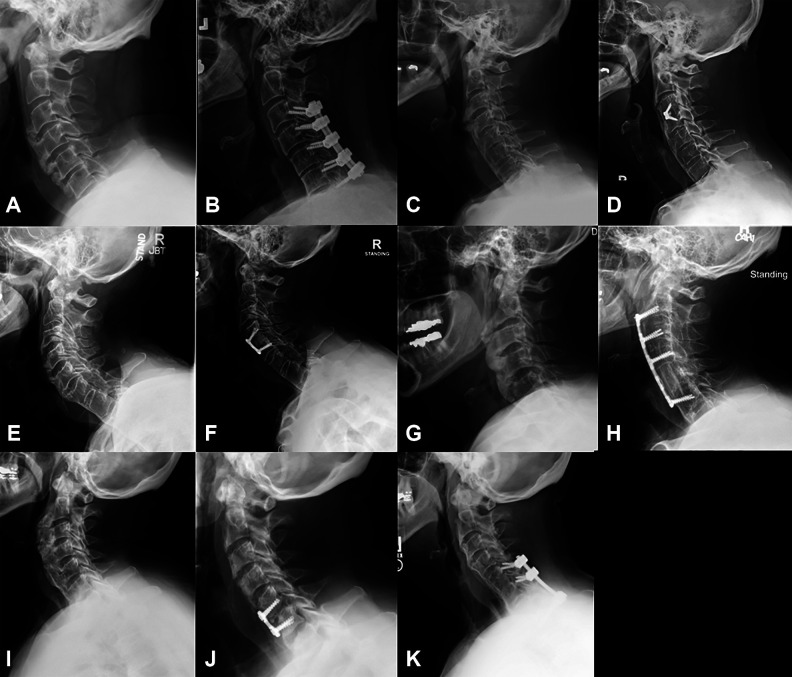
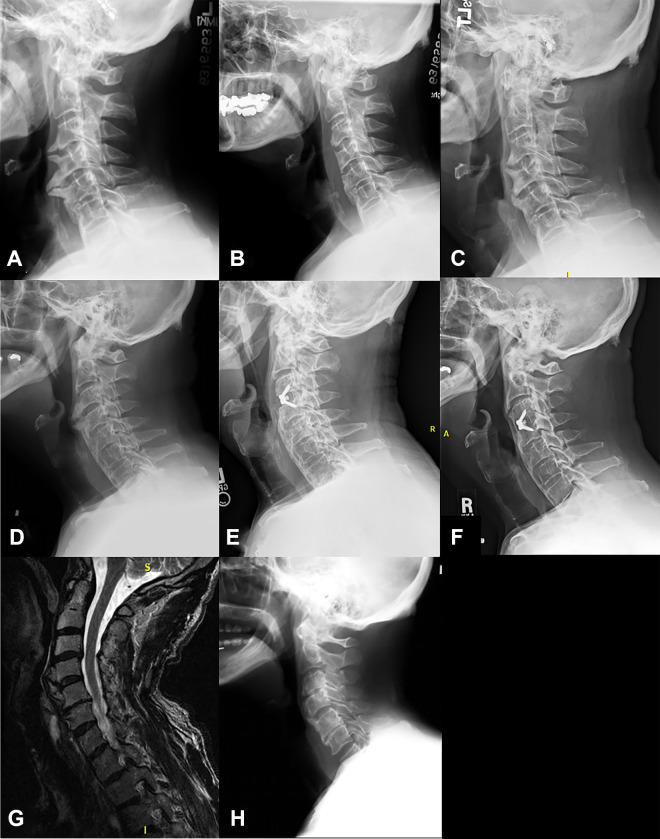
Methods: Retrospective review identified 19 patients who underwent anterior cervical osteophyte resection for a diagnosis of dysphagia. The mean age was 71 years and follow-up, 4.7 years. The most common level operated on was C3-C4 (13, 69%).
Results: Following anterior cervical osteophyte resection, 79% of patients had improvement in dysphagia. Five patients underwent cervical fusion; there were no episodes of delayed or iatrogenic instability requiring fusion. Fusion patients were younger (64 vs 71 years, P = .05) and had longer operative times (315 vs 121 minutes, P = .01). Age of 75 years or less trended toward improvement in dysphagia (P = .09; OR = 18.8; 95% CI 0.7-478.0), whereas severe dysphagia trended toward increased complications (P = .07; OR = 11.3; 95% CI = 0.8-158.5). Body mass index, use of an exposure surgeon, diffuse idiopathic skeletal hyperostosis diagnosis, surgery at 3 or more levels, prior neck surgery, and fusion were not predictive of improvement or complication.
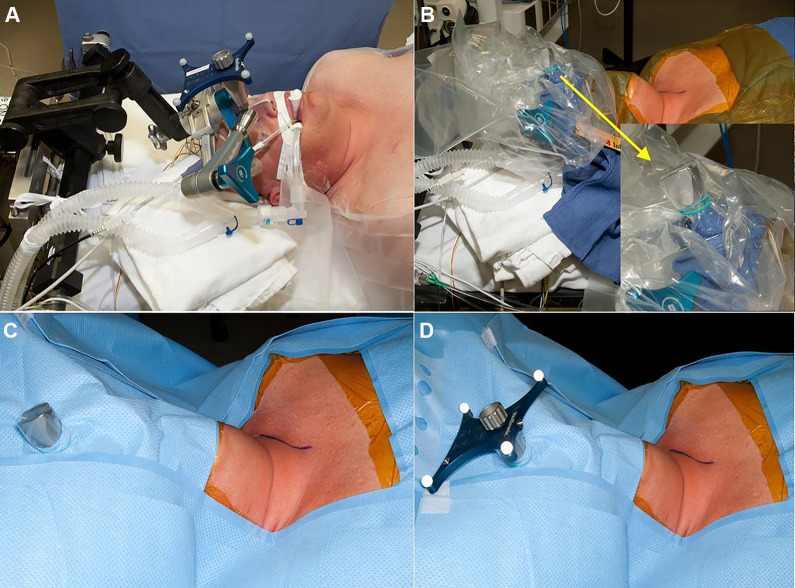
Conclusions: Anterior cervical osteophyte resection improves swallowing function in the majority of patients with symptomatic osteophytes. Spinal fusion can be added to address stenosis and other underlying cervical disease and help prevent osteophyte recurrence, whereas intraoperative navigation can be used to ensure complete osteophyte resection without breaching the cortex or entering the disc space. Because of the relatively high complication rate, patients should undergo thorough multidisciplinary workup with swallow evaluation to confirm that anterior cervical osteophytes are the primary cause of dysphagia prior to surgery.
Keywords: DISH; cervical spine; cheilectomy; dysphagia; osteophyte; syndesmophyte.
Conflict of interest statement
Figures
References
-
- Parker MD. Dysphagia due to cervical osteophytes: a controversial entity revisited. Dysphagia. 1989;3:157–160. - PubMed
-
- Klaassen Z, Tubbs RS, Apaydin N, Hage R, Jordan R, Loukas M. Vertebral spinal osteophytes. Anat Sci Int. 2011;86:1–9. doi:10.1007/s12565-010-0080-8 - PubMed
-
- Vodicar M, Kosak R, Vengust R. Long-term results of surgical treatment for symptomatic anterior cervical osteophytes: a case series with review of the literature. Clin Spine Surg. 2016;29:E482–E487. doi:10.1097/BSD.0b013e31829046af - PubMed
-
- Resnick D, Niwayama G. Radiographic and pathologic features of spinal involvement in diffuse idiopathic skeletal hyperostosis (DISH). Radiology. 1976;119:559–568. doi:10.1148/119.3.559 - PubMed
-
- Strasser G, Schima W, Schober E, Pokieser P, Kaider A, Denk DM. Cervical osteophytes impinging on the pharynx: importance of size and concurrent disorders for development of aspiration. AJR Am J Roentgenol. 2000;174:449–453. doi:10.2214/ajr.174.2.1740449 - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
