

Derivation and Validation of Novel Phenotypes of Multiple Organ Dysfunction Syndrome in Critically Ill Children
- PMID: 32780121
- PMCID: PMC7420303
- DOI: 10.1001/jamanetworkopen.2020.9271
Derivation and Validation of Novel Phenotypes of Multiple Organ Dysfunction Syndrome in Critically Ill Children
Abstract
Importance: Multiple organ dysfunction syndrome (MODS) is a dynamic and heterogeneous process associated with high morbidity and mortality in critically ill children.
Objective: To determine whether data-driven phenotypes of MODS based on the trajectories of 6 organ dysfunctions have prognostic and therapeutic relevance in critically ill children.
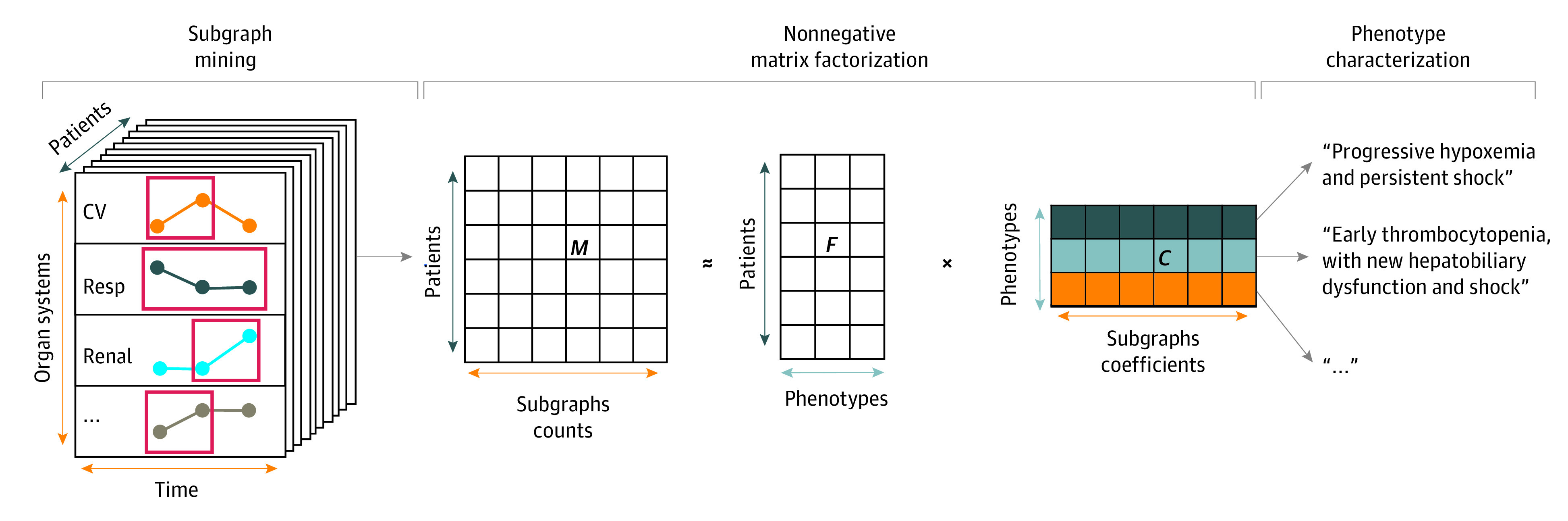
Design, setting, and participants: This cohort study included 20 827 pediatric intensive care encounters among 14 285 children admitted to 2 large academic pediatric intensive care units (PICUs) between January 2010 and August 2016. Patients were excluded if they were older than 21 years or had undergone cardiac surgery. The 6 subscores of the pediatric Sequential Organ Failure Assessment (pSOFA) score were calculated for the first 3 days, including the subscores for respiratory, cardiovascular, coagulation, hepatic, neurologic, and renal dysfunctions. MODS was defined as a pSOFA subscore of at least 2 in at least 2 organs. Encounters were split in a 80:20 ratio for derivation and validation, respectively. The trajectories of the 6 subscores were used to derive a set of data-driven phenotypes of MODS using subgraph-augmented nonnegative matrix factorization in the derivation set. Data analysis was conducted from March to October 2019.
Exposures: The primary exposure was phenotype membership. In the subset of patients with vasoactive-dependent shock, the interaction between hydrocortisone and phenotype membership and its association with outcomes were examined in a matched cohort.
Main outcomes and measures: The primary outcome was in-hospital mortality. Secondary outcomes included persistent MODS on day 7, and vasoactive-free, ventilator-free, and hospital-free days. Regression analysis was used to adjust for age, severity of illness, immunocompromised status, and study site.
Results: There were 14 285 patients with 20 827 encounters (median [interquartile range] age 5.2 years [1.5-12.7] years; 11 409 [54.8%; 95% CI, 54.1%-55.5%] male patients). Of these, 5297 encounters (25.4%; 95% CI, 24.8%-26.0%) were with patients who had MODS, of which 5054 (95.4%) met the subgraph count threshold and were included in the analysis. Subgraph augmented nonnegative matrix factorization uncovered 4 data-driven phenotypes of MODS, characterized by a combination of neurologic, respiratory, coagulation, and cardiovascular dysfunction, as follows: phenotype 1, severe, persistent encephalopathy (1019 patients [19.2%]); phenotype 2, moderate, resolving hypoxemia (1828 patients [34.5%]); phenotype 3, severe, persistent hypoxemia and shock (1012 patients [19.1%]); and phenotype 4, moderate, persistent thrombocytopenia and shock (1195 patients [22.6%]). These phenotypes were reproducible in a validation set of encounters, had distinct clinical characteristics, and were independently associated with outcomes. For example, using phenotype 2 as reference, the adjusted hazard ratios (aHRs) for death by 28 days were as follows: phenotype 1, aHR of 3.0 (IQR, 2.1-4.3); phenotype 3, aHR of 2.8 (IQR, 2.0-4.1); and phenotype 4, aHR of 1.8 (IQR, 1.2-2.6). Interaction analysis in a matched cohort of patients with vasoactive-dependent shock revealed that hydrocortisone had differential treatment association with vasoactive-free days across phenotypes. For example, patients in phenotype 3 who received hydrocortisone had more vasoactive-free days than those who did not (23 days vs 18 days; P for interaction < .001), whereas patients in other phenotypes who received hydrocortisone either had no difference or had less vasoactive-free days.
Conclusions and relevance: In this study, data-driven phenotyping in critically ill children with MODS uncovered 4 distinct and reproducible phenotypes with prognostic relevance and possible therapeutic relevance. Further validation and characterization of these phenotypes is warranted.
Conflict of interest statement
Figures

Similar articles
-
Adaptation and Validation of a Pediatric Sequential Organ Failure Assessment Score and Evaluation of the Sepsis-3 Definitions in Critically Ill Children.JAMA Pediatr. 2017 Oct 2;171(10):e172352. doi: 10.1001/jamapediatrics.2017.2352. Epub 2017 Oct 2. JAMA Pediatr. 2017. PMID: 28783810 Free PMC article.
-
Biomarker Assessment of a High-Risk, Data-Driven Pediatric Sepsis Phenotype Characterized by Persistent Hypoxemia, Encephalopathy, and Shock.Pediatr Crit Care Med. 2024 Jun 1;25(6):512-517. doi: 10.1097/PCC.0000000000003499. Epub 2024 Mar 11. Pediatr Crit Care Med. 2024. PMID: 38465952 Free PMC article.
-
Derivation and Validation of Vasoactive Inotrope Score Trajectory Groups in Critically Ill Children With Shock.Pediatr Crit Care Med. 2022 Dec 1;23(12):1017-1026. doi: 10.1097/PCC.0000000000003070. Epub 2022 Sep 2. Pediatr Crit Care Med. 2022. PMID: 36053068 Free PMC article.
-
The pediatric multiple organ dysfunction syndrome.Pediatr Crit Care Med. 2009 Jan;10(1):12-22. doi: 10.1097/PCC.0b013e31819370a9. Pediatr Crit Care Med. 2009. PMID: 19057438 Review.
-
Severity of illness and organ dysfunction scoring in children.Pediatr Crit Care Med. 2005 May;6(3 Suppl):S126-34. doi: 10.1097/01.PCC.0000161287.61028.D4. Pediatr Crit Care Med. 2005. PMID: 15857545 Review.
Cited by
-
The brain in pediatric critical care: unique aspects of assessment, monitoring, investigations, and follow-up.Intensive Care Med. 2022 May;48(5):535-547. doi: 10.1007/s00134-022-06683-4. Epub 2022 Apr 21. Intensive Care Med. 2022. PMID: 35445823 Free PMC article. Review.
-
Application of AI and IoT in Clinical Medicine: Summary and Challenges.Curr Med Sci. 2021 Dec;41(6):1134-1150. doi: 10.1007/s11596-021-2486-z. Epub 2021 Dec 22. Curr Med Sci. 2021. PMID: 34939144 Free PMC article.
-
Accurate long-term prediction of death for patients with cirrhosis.Hepatology. 2022 Sep;76(3):700-711. doi: 10.1002/hep.32457. Epub 2022 Apr 1. Hepatology. 2022. PMID: 35278226 Free PMC article.
-
Commentary: 'Critical illness subclasses: all roads lead to Rome'.Crit Care. 2022 Dec 14;26(1):387. doi: 10.1186/s13054-022-04265-w. Crit Care. 2022. PMID: 36517867 Free PMC article. No abstract available.
-
Sepsis subphenotyping based on organ dysfunction trajectory.Crit Care. 2022 Jul 3;26(1):197. doi: 10.1186/s13054-022-04071-4. Crit Care. 2022. PMID: 35786445 Free PMC article.
References
-
- Tamburro RF, Jenkins TL. Multiple organ dysfunction syndrome: a challenge for the pediatric critical care community. Pediatr Crit Care Med. 2017;18(3_suppl)(suppl 1):S1-S3. - PubMed
-
- Lin JC, Spinella PC, Fitzgerald JC, et al. ; Sepsis Prevalence, Outcomes, and Therapy Study Investigators . New or progressive multiple organ dysfunction syndrome in pediatric severe sepsis: a sepsis phenotype with higher morbidity and mortality. Pediatr Crit Care Med. 2017;18(1):8-16. doi:10.1097/PCC.0000000000000978 - DOI - PMC - PubMed
-
- Leteurtre S, Duhamel A, Deken V, Lacroix J, Leclerc F; Groupe Francophone de Réanimation et Urgences Pédiatriques . Daily estimation of the severity of organ dysfunctions in critically ill children by using the PELOD-2 score. Crit Care. 2015;19:324. doi:10.1186/s13054-015-1054-y - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
