

Adolescent idiopathic scoliosis detection and referral trends: impact treatment options
- PMID: 32780304
- PMCID: PMC7775861
- DOI: 10.1007/s43390-020-00182-6
Adolescent idiopathic scoliosis detection and referral trends: impact treatment options
Abstract
Study design: Retrospective cross-sectional study.
Objective: To analyze the patient demographic referred for scoliosis to the Hospital for Sick Children to determine the proportion of patients suitable for brace treatment, as per the Scoliosis Research Society guidelines. There is level 1 evidence that bracing in adolescent idiopathic scoliosis (AIS) decreases the risk of curve progression and need for surgery, but optimal brace treatment requires early curve detection.
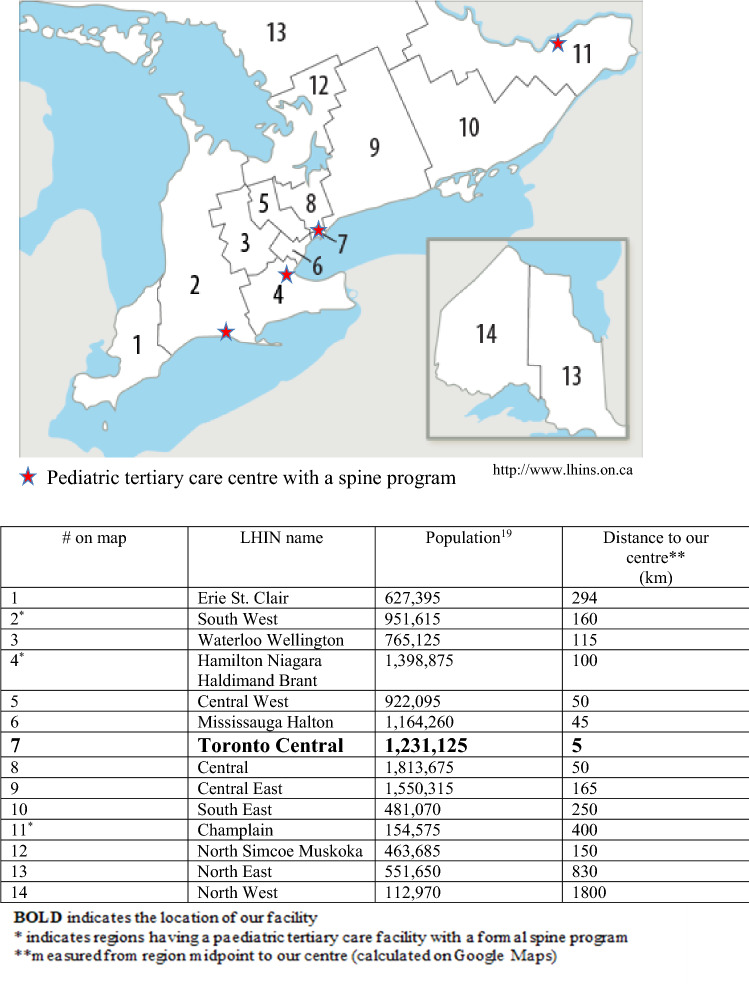
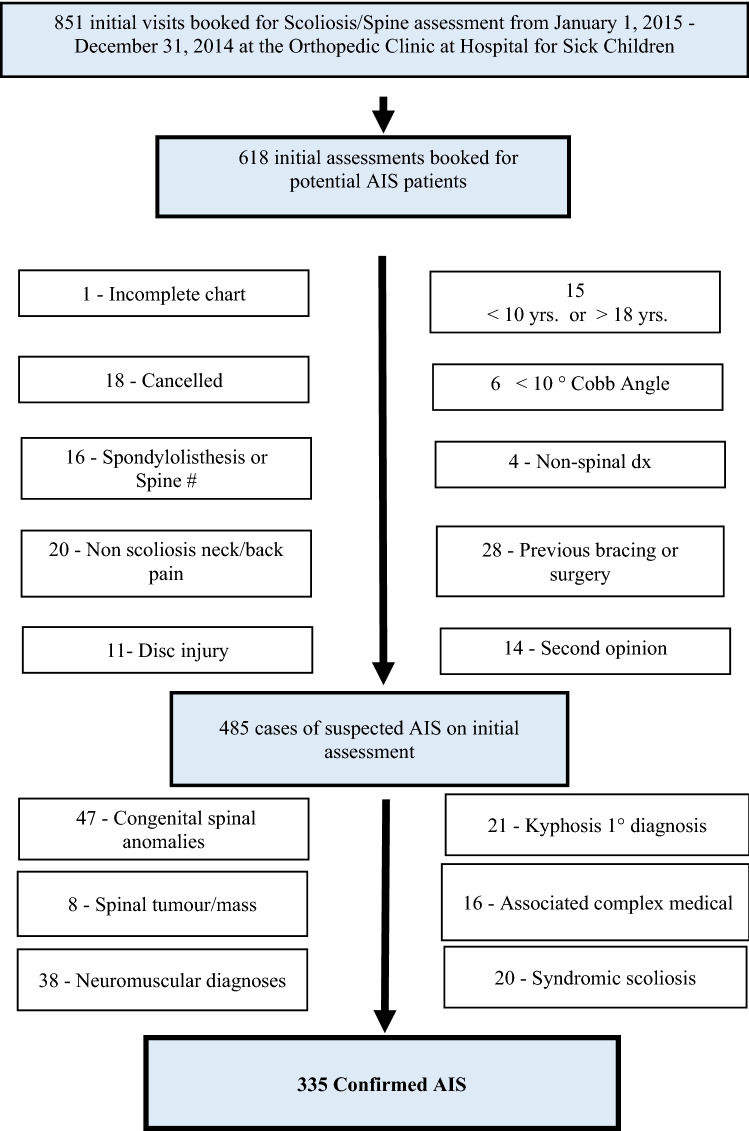
Methods: We performed a retrospective review of 618 consecutive patients who underwent initial assessment in our Spine Clinic between Jan. 1 and Dec. 31, 2014. We included children 10-18 years, with scoliosis greater than 10°, excluding those diagnosed with non-idiopathic curves. Primary outcomes were Cobb angle, menarchal status, and Risser score. We analyzed the effect of specific referral variables (family history, the person who first noticed the curve, and geographic location of residence) on presenting curve magnitude.
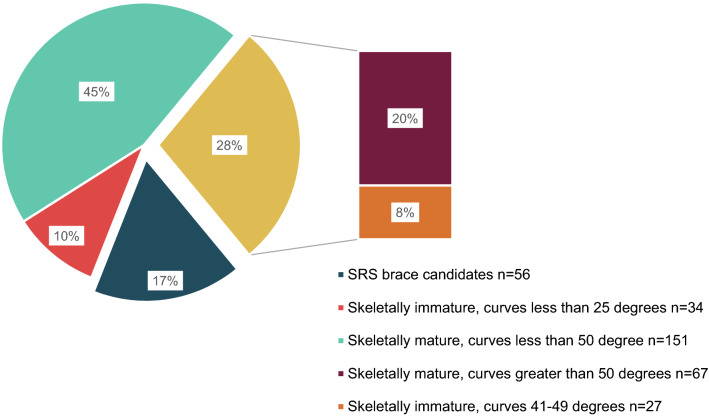
Results: During the study period, 335 children met the inclusion criteria, with an average age of 14.1 ± 1.8 years and a mean Cobb angle of 36.8 ± 14.5°. Brace treatment was indicated in 17% of patients; 18% had curves beyond optimal curve range for bracing (> 40°), and 55% were skeletally mature, therefore not brace candidates. The majority of curves (54%) were first detected by the patient or family member and averaged 7° more than curves first detected by a physician. A family history of scoliosis made no difference to curve magnitude, nor did geographic location of residence.
Conclusion: The majority of AIS patients present too late for effective management with bracing.
Level of evidence: III.
Keywords: Adolescent idiopathic scoliosis; Appropriateness of care; Brace treatment; Pediatric; Referral pattern.
Conflict of interest statement
Dr. Zeller receives royalties from SpineVision® (excluding personal use) and is an unpaid consultant for Paradigm Spine, LLC. The authors declare that there are no financial, general, or institutional competing interests in relation to this research paper being accepted for publication.
Figures

References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous