

Sleeping Beauty-engineered CAR T cells achieve antileukemic activity without severe toxicities
- PMID: 32780725
- PMCID: PMC7598053
- DOI: 10.1172/JCI138473
Sleeping Beauty-engineered CAR T cells achieve antileukemic activity without severe toxicities
Abstract
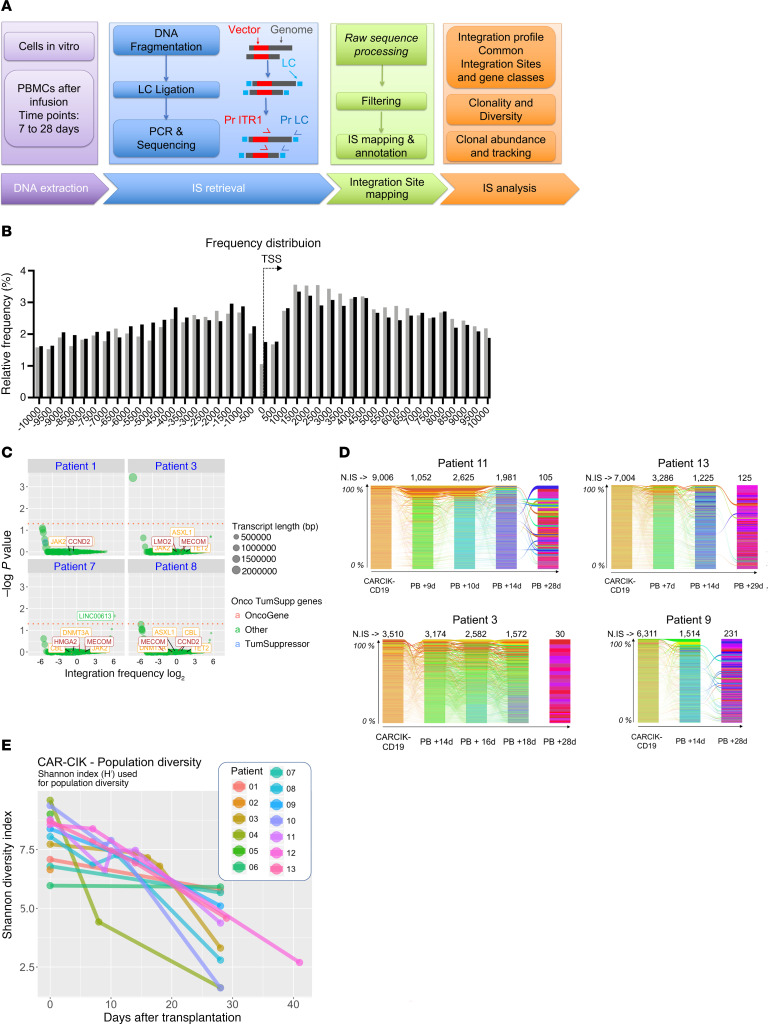
BACKGROUNDChimeric antigen receptor (CAR) T cell immunotherapy has resulted in complete remission (CR) and durable response in highly refractory patients. However, logistical complexity and high costs of manufacturing autologous viral products limit CAR T cell availability.METHODSWe report the early results of a phase I/II trial in B cell acute lymphoblastic leukemia (B-ALL) patients relapsed after allogeneic hematopoietic stem cell transplantation (HSCT) using donor-derived CD19 CAR T cells generated with the Sleeping Beauty (SB) transposon and differentiated into cytokine-induced killer (CIK) cells.RESULTSThe cellular product was produced successfully for all patients from the donor peripheral blood (PB) and consisted mostly of CD3+ lymphocytes with 43% CAR expression. Four pediatric and 9 adult patients were infused with a single dose of CAR T cells. Toxicities reported were 2 grade I and 1 grade II cytokine-release syndrome (CRS) cases at the highest dose in the absence of graft-versus-host disease (GVHD), neurotoxicity, or dose-limiting toxicities. Six out of 7 patients receiving the highest doses achieved CR and CR with incomplete blood count recovery (CRi) at day 28. Five out of 6 patients in CR were also minimal residual disease negative (MRD-). Robust expansion was achieved in the majority of the patients. CAR T cells were measurable by transgene copy PCR up to 10 months. Integration site analysis showed a positive safety profile and highly polyclonal repertoire in vitro and at early time points after infusion.CONCLUSIONSB-engineered CAR T cells expand and persist in pediatric and adult B-ALL patients relapsed after HSCT. Antileukemic activity was achieved without severe toxicities.TRIAL REGISTRATIONClinicalTrials.gov NCT03389035.FUNDINGThis study was supported by grants from the Fondazione AIRC per la Ricerca sul Cancro (AIRC); Cancer Research UK (CRUK); the Fundación Científica de la Asociación Española Contra el Cáncer (FC AECC); Ministero Della Salute; Fondazione Regionale per la Ricerca Biomedica (FRRB).
Keywords: Cancer gene therapy; Clinical Trials; Hematology; Immunotherapy; Leukemias.
Conflict of interest statement
Figures





References
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
