

Development and validation of a prediction model for severe respiratory failure in hospitalized patients with SARS-CoV-2 infection: a multicentre cohort study (PREDI-CO study)
- PMID: 32781244
- PMCID: PMC7414420
- DOI: 10.1016/j.cmi.2020.08.003
Development and validation of a prediction model for severe respiratory failure in hospitalized patients with SARS-CoV-2 infection: a multicentre cohort study (PREDI-CO study)
Erratum in
-
Corrigendum to: "Development and validation of a prediction model for severe respiratory failure in hospitalized patients with SARS-CoV-2 infection: a multicentre cohort study (PREDI-CO study)" Clinical Microbiology and Infection 26 (2020) 1545-1553.Clin Microbiol Infect. 2023 Jun;29(6):817. doi: 10.1016/j.cmi.2023.02.017. Epub 2023 Mar 1. Clin Microbiol Infect. 2023. PMID: 36868355 Free PMC article. No abstract available.
Abstract
Objectives: We aimed to develop and validate a risk score to predict severe respiratory failure (SRF) among patients hospitalized with coronavirus disease-2019 (COVID-19).
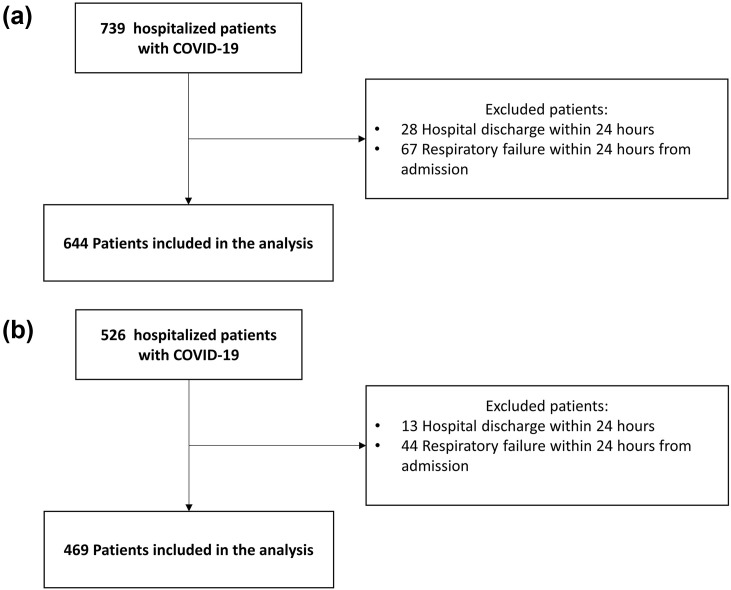
Methods: We performed a multicentre cohort study among hospitalized (>24 hours) patients diagnosed with COVID-19 from 22 February to 3 April 2020, at 11 Italian hospitals. Patients were divided into derivation and validation cohorts according to random sorting of hospitals. SRF was assessed from admission to hospital discharge and was defined as: Spo2 <93% with 100% Fio2, respiratory rate >30 breaths/min or respiratory distress. Multivariable logistic regression models were built to identify predictors of SRF, β-coefficients were used to develop a risk score. Trial Registration NCT04316949.
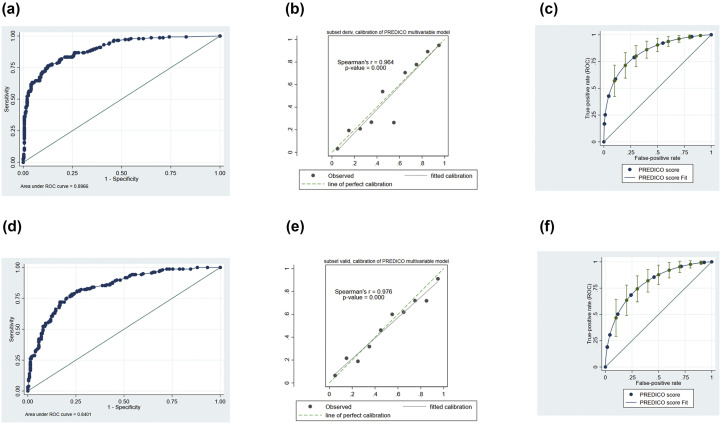
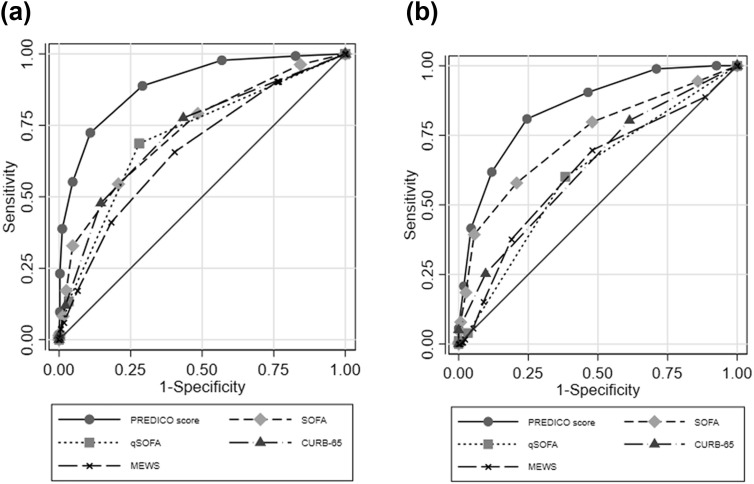
Results: We analysed 1113 patients (644 derivation, 469 validation cohort). Mean (±SD) age was 65.7 (±15) years, 704 (63.3%) were male. SRF occurred in 189/644 (29%) and 187/469 (40%) patients in the derivation and validation cohorts, respectively. At multivariate analysis, risk factors for SRF in the derivation cohort assessed at hospitalization were age ≥70 years (OR 2.74; 95% CI 1.66-4.50), obesity (OR 4.62; 95% CI 2.78-7.70), body temperature ≥38°C (OR 1.73; 95% CI 1.30-2.29), respiratory rate ≥22 breaths/min (OR 3.75; 95% CI 2.01-7.01), lymphocytes ≤900 cells/mm3 (OR 2.69; 95% CI 1.60-4.51), creatinine ≥1 mg/dL (OR 2.38; 95% CI 1.59-3.56), C-reactive protein ≥10 mg/dL (OR 5.91; 95% CI 4.88-7.17) and lactate dehydrogenase ≥350 IU/L (OR 2.39; 95% CI 1.11-5.11). Assigning points to each variable, an individual risk score (PREDI-CO score) was obtained. Area under the receiver-operator curve was 0.89 (0.86-0.92). At a score of >3, sensitivity, specificity, and positive and negative predictive values were 71.6% (65%-79%), 89.1% (86%-92%), 74% (67%-80%) and 89% (85%-91%), respectively. PREDI-CO score showed similar prognostic ability in the validation cohort: area under the receiver-operator curve 0.85 (0.81-0.88). At a score of >3, sensitivity, specificity, and positive and negative predictive values were 80% (73%-85%), 76% (70%-81%), 69% (60%-74%) and 85% (80%-89%), respectively.
Conclusion: PREDI-CO score can be useful to allocate resources and prioritize treatments during the COVID-19 pandemic.
Keywords: Age; C-reactive proteine; Coronavirus disease 2019; Lactate dehydrogenase; Obesity; Prognostic tool; Severe acute respiratory syndrome coronavirus 2; Severe respiratory failure.
Copyright © 2020 European Society of Clinical Microbiology and Infectious Diseases. Published by Elsevier Ltd. All rights reserved.
Figures
References
-
- Wu Z., McGoogan J.M. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72314 cases from the Chinese center for disease control and prevention. JAMA. 2020 epub ahead of print. - PubMed
-
- Grasselli G., Pesenti A., Cecconi M. Critical Care utilization for the COVID-19 outbreak in Lombardy, Italy: early experience and forecast during an emergency response. JAMA. 2020 epub ahead of print. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
