

Recurrent small bowel obstruction caused by Burkitt lymphoma in an elderly man: a case report and review of the literature
- PMID: 32782017
- PMCID: PMC7422579
- DOI: 10.1186/s13256-020-02449-y
Recurrent small bowel obstruction caused by Burkitt lymphoma in an elderly man: a case report and review of the literature
Abstract
Background: Acute small bowel obstruction is a common surgical emergency usually caused by abdominal adhesions, followed by intraluminal tumors from metastatic disease. Although lymphomas have been known to cause bowel obstruction, Burkitt lymphoma is seldom reported to induce an obstruction in the adult population.
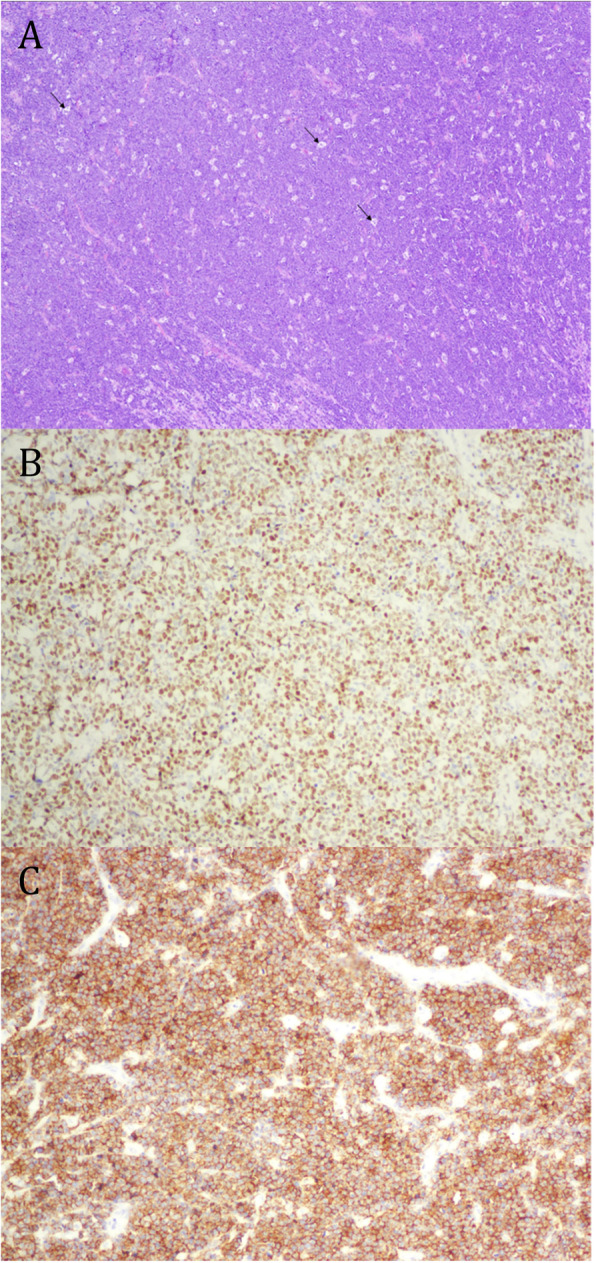
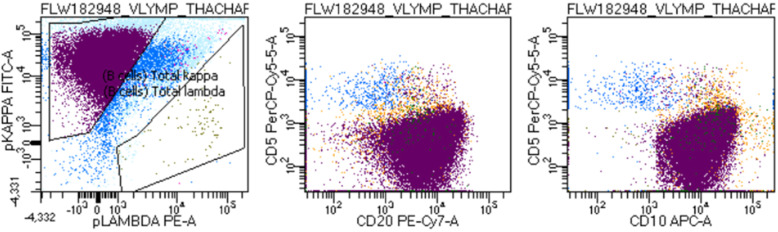
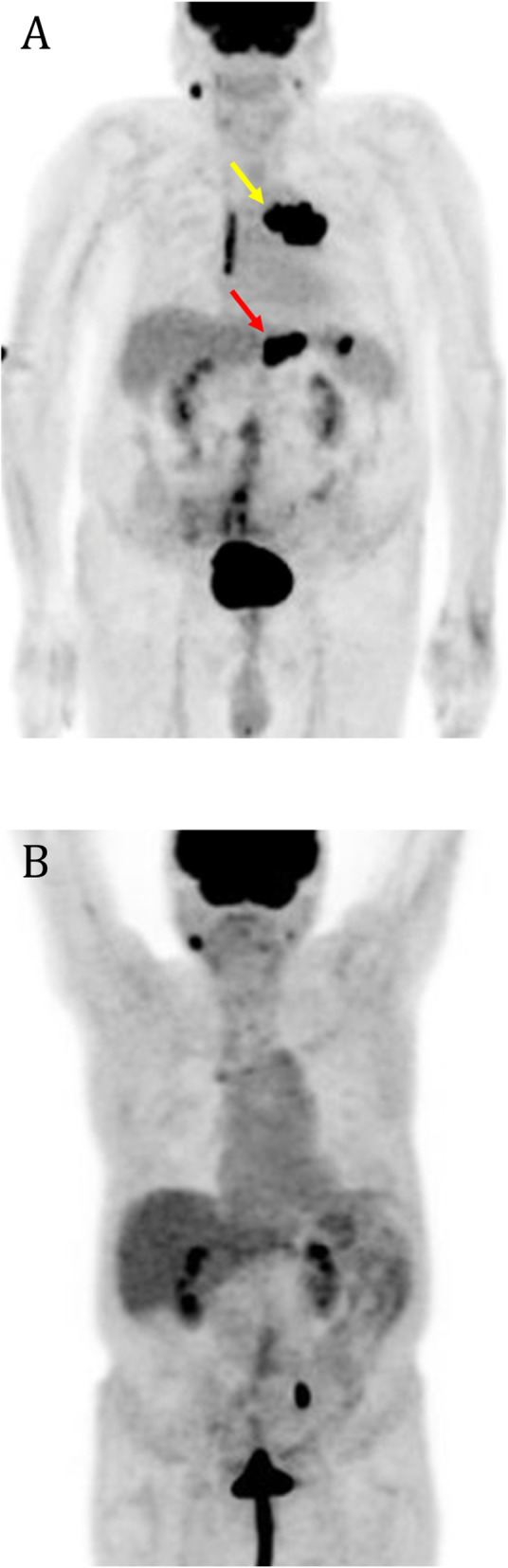
Case presentation: A 78-year-old Hispanic man with a history of abdominal interventions presented to our hospital with abdominal pain. Computed tomography revealed a partial small bowel obstruction attributed to local inflammation or adhesions. Medical management with bowel rest and nasogastric decompression resulted in resolution of symptoms and quick discharge. He returned 2 days later with worsening abdominal pain. Repeat imaging showed progression of the partial small bowel obstruction, but with an additional 1.6-cm nodular density abutting the anterior aspect of the gastric antrum and lobulated anterior gastric antral wall thickening. He was taken to the operating room, where several masses were found. Intraoperative frozen sections were consistent with lymphoma, and pathology later revealed Burkitt lymphoma. Disease was found on both sides of the diaphragm by positron emission tomography. After the initial resection and adjuvant chemotherapy, the patient is alive and well about 14 months after resection.
Conclusions: Small bowel obstruction is uncommonly due to Burkitt lymphoma in the geriatric population and is more frequently seen in the pediatric and young adult populations. Burkitt lymphoma is very aggressive with rapid cell turnover leading to significant morbidity. The rapid recurrence of an acute abdominal process should prompt an investigation for a more sinister cause such as malignancy.
Keywords: Recurrent; Small bowel obstruction; Sporadic Burkitt lymphoma.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
