

Wearable monitoring of sleep-disordered breathing: estimation of the apnea-hypopnea index using wrist-worn reflective photoplethysmography
- PMID: 32782313
- PMCID: PMC7421543
- DOI: 10.1038/s41598-020-69935-7
Wearable monitoring of sleep-disordered breathing: estimation of the apnea-hypopnea index using wrist-worn reflective photoplethysmography
Abstract
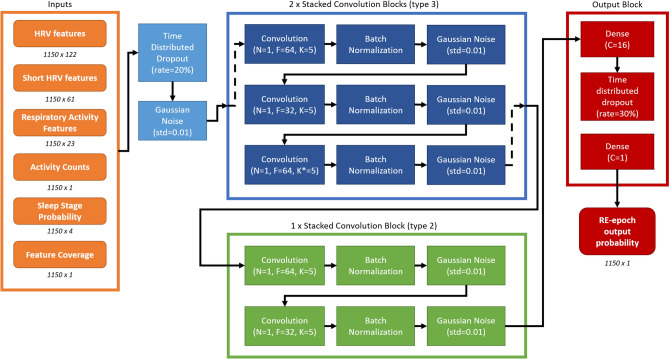
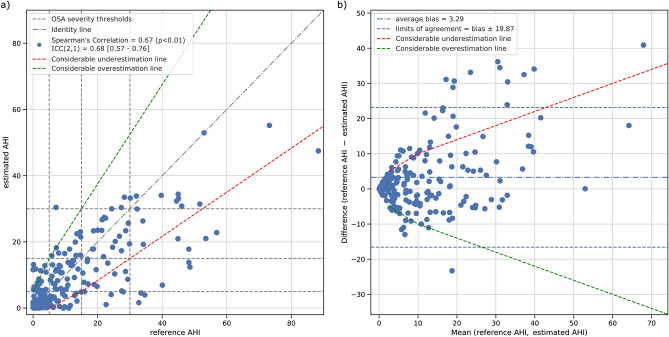
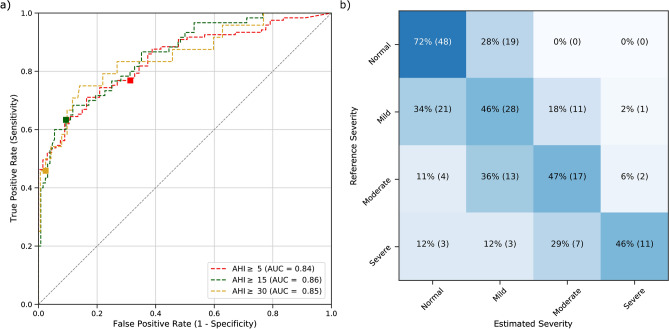
A large part of the worldwide population suffers from obstructive sleep apnea (OSA), a disorder impairing the restorative function of sleep and constituting a risk factor for several cardiovascular pathologies. The standard diagnostic metric to define OSA is the apnea-hypopnea index (AHI), typically obtained by manually annotating polysomnographic recordings. However, this clinical procedure cannot be employed for screening and for long-term monitoring of OSA due to its obtrusiveness and cost. Here, we propose an automatic unobtrusive AHI estimation method fully based on wrist-worn reflective photoplethysmography (rPPG), employing a deep learning model exploiting cardiorespiratory and sleep information extracted from the rPPG signal trained with 250 recordings. We tested our method with an independent set of 188 heterogeneously disordered clinical recordings and we found it estimates the AHI with a good agreement to the gold standard polysomnography reference (correlation = 0.61, estimation error = 3±10 events/h). The estimated AHI was shown to reliably assess OSA severity (weighted Cohen's kappa = 0.51) and screen for OSA (ROC-AUC = 0.84/0.86/0.85 for mild/moderate/severe OSA). These findings suggest that wrist-worn rPPG measurements that can be implemented in wearables such as smartwatches, have the potential to complement standard OSA diagnostic techniques by allowing unobtrusive sleep and respiratory monitoring.
Conflict of interest statement
P.F. declares to be employed by Philips Research. The employer had no influence on the study and on the decision to publish. G.B.P. is a PhD student, fully employed by the Eindhoven University of Technology, with a guest status with Sleep Medicine Centre Kempenhaeghe and Philips Research, in order to have access to data and tools within the collaboration. J.W.M.B. is an academic advisor at Philips Research. The other authors declare no competing interests.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
