

Diverse activation patterns during persistent atrial fibrillation by noncontact charge-density mapping of human atrium
- PMID: 32782641
- PMCID: PMC7411208
- DOI: 10.1002/joa3.12361
Diverse activation patterns during persistent atrial fibrillation by noncontact charge-density mapping of human atrium
Abstract
Background: Global simultaneous recording of atrial activation during atrial fibrillation (AF) can elucidate underlying mechanisms contributing to AF maintenance. A better understanding of these mechanisms may allow for an individualized ablation strategy to treat persistent AF. The study aims to characterize left atrial endocardial activation patterns during AF using noncontact charge-density mapping.
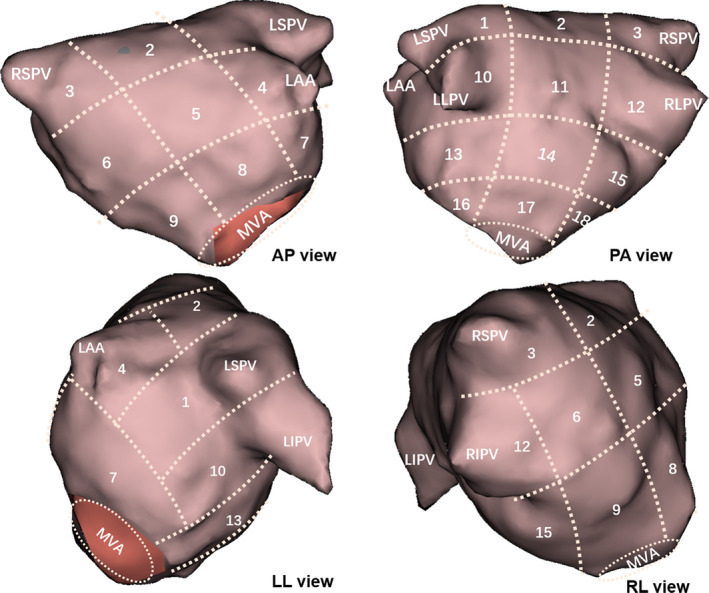
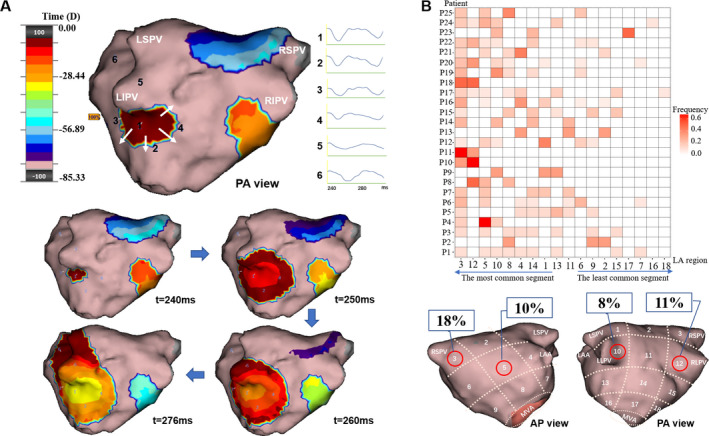
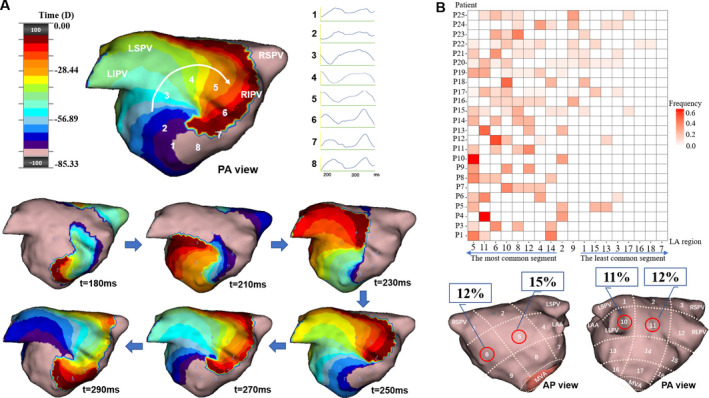
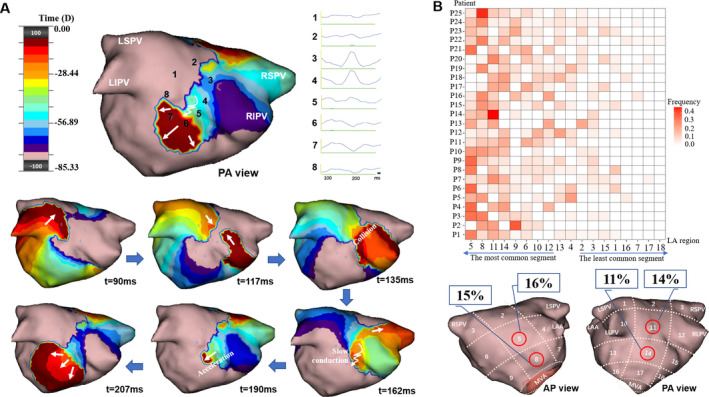
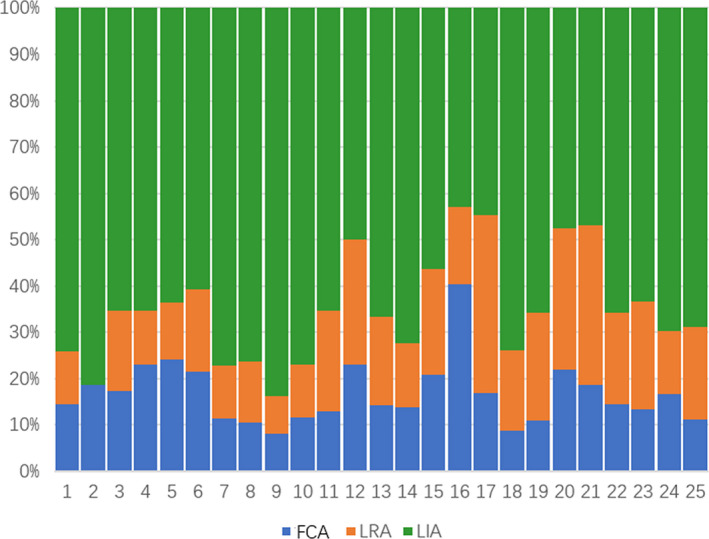
Methods: Twenty-five patients with persistent AF were studied. Activation patterns were characterized into three subtypes: (i) focal with centrifugal activation (FCA); (ii) localized rotational activation (LRA); and (iii) localized irregular activation (LIA). Continuous activation patterns were analyzed and distributed in 18 defined regions in the left atrium.
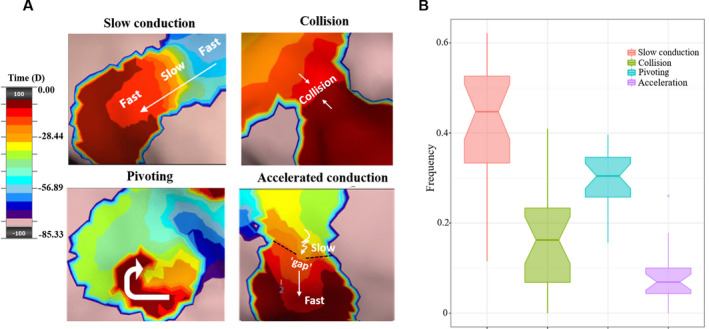
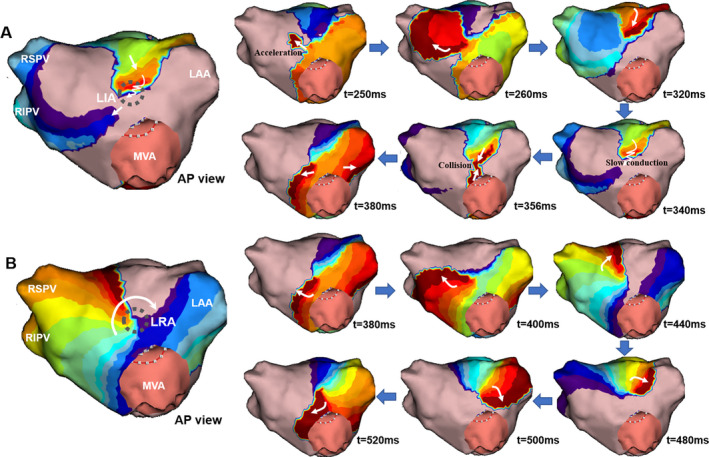
Results: A total of 144 AF segments with 1068 activation patterns were analyzed. The most common pattern during AF was LIA (63%) which consists of four disparate features of activation: slow conduction (45%), pivoting (30%), collision (16%), and acceleration (7%). LRA was the second-most common pattern (20%). FCA accounted for 17% of all activations, arising frequently from the pulmonary veins (PVs)/ostia. A majority of patients (24/25; 96%) showed continuous and highly dynamic patterns of activation comprising multiple combinations of FCA, LRA, and LIA, transitioning from one to the other without a discernible order. Preferential conduction areas were typically seen in the mid-anterior (48%) and lower-posterior (40%) walls.
Conclusion: Atrial fibrillation is characterized by heterogeneous activation patterns identified in PV-ostia and non-PV regions throughout the LA at varying locations between individuals. Clinical implications of individualized ablation strategies guided by charge-density mapping need to be determined.
Keywords: activation pattern; atrial fibrillation; localized irregular activation; localized rotational activation; noncontact charge‐density mapping.
© 2020 The Authors. Journal of Arrhythmia published by John Wiley & Sons Australia, Ltd on behalf of the Japanese Heart Rhythm Society.
Figures
References
-
- Haïssaguerre M, Jaïs P, Shah DC, Takahashi A, Hocini M, Quiniou G, et al. Spontaneous initiation of atrial fibrillation by ectopic beats originating in the pulmonary veins. N Engl J Med. 1998;339:659–66. - PubMed
-
- Verma A, Jiang C‐Y, Betts TR, Chen J, Deisenhofer I, Mantovan R, et al. Approaches to catheter ablation for persistent atrial fibrillation. N Engl J Med. 2015;372:1812–22. - PubMed
-
- Vogler J, Willems S, Sultan A, Schreiber D, Lüker J, Servatius H, et al. Pulmonary vein isolation versus defragmentation: the CHASE‐AF clinical trial. J Am Coll Cardiol. 2015;66:2743–52. - PubMed
-
- Narayan SM, Krummen DE, Shivkumar K, Clopton P, Rappel W‐J, Miller JM, et al. Treatment of atrial fibrillation by the ablation of localized sources: CONFIRM (Conventional Ablation for Atrial Fibrillation With or Without Focal Impulse and Rotor Modulation) trial. J Am Coll Cardiol. 2012;60:628–36. - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
